ATTD 2021 was held 2-5 June, 2021 and, thanks to dedoc, I had the privilege to attend and live tweet the presentations. However, with many sessions running in parallel, it was not possible to attend every session and many sessions covered similar topics. To address this, I watched the recordings of the sessions I missed and brought them together under common themes. Where the presentation called out that the results were confidential and/or not yet published and not for distribution I left them out of my blog but I can confirm there was nothing presented under confidence which contradicted what I am presenting in these summaries.
This is my second “distillation” which is on pregnancy and gestational diabetes. For my first “distillation” covering looping go here. Firstly, let me be clear in my intent: I am a male and never been pregnant. My aim is to present the research, as I understand it, from ATTD 2021. I am not a medical professional and nothing here should be considered medical advice or me telling you what to do with your body. If something I have written is of interest, I strongly encourage you to discuss it with your medical team to determine the best course of action for you. I will also call out that this post discusses the possible adverse outcomes of pregnancy for the baby. Not all pregnancies go to plan and if this subject is distressing for you, you may be triggered by the contents of this post.
A common observation of women with diabetes is their menstrual cycle has a significant impact on their blood glucose level management. It is known in that the fluctuation of hormone levels in the body directly impacts insulin resistance. The same happens in pregnancy with the thinking being that hormone levels increase in a woman’s body to increase insulin resistance so more glucose reaches the baby for growth and development.
For women with diabetes this amplifies an existing health condition and, for women who do not have diabetes, given the stresses this puts the body under, it can trigger diabetes during pregnancy in what is called Gestational Diabetes. ATTD 2021 looked at some of the latest research on diabetes and pregnancy which I present here.
Specific questions covered in the presentations were:
- If I am a Woman with Diabetes, What are the Health Risks to my Baby?
- Health Benefits of Using a CGM During Pregnancy
- Should Women with Diabetes Take Metformin?
As usual there is a TL;DR section at the end if you want to read the summary of results without the details.
If I am a Woman with Diabetes, What are the Health Risks to my Baby?
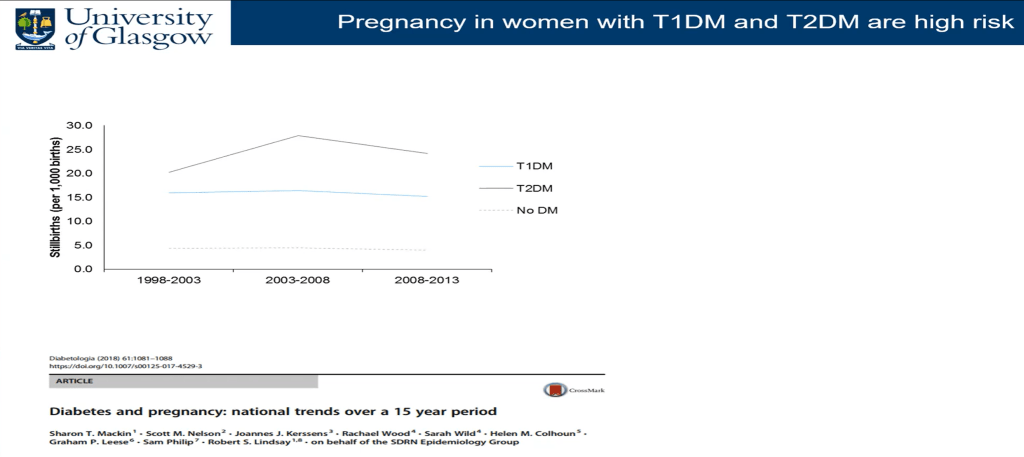
Dr. Helen Murphy presented on the risks to the baby for women with Type 1 and Type 2 diabetes. Both Dr. Murphy and other presenters made it clear that there has not been a lot of improvement in adverse outcomes for pregnant women with diabetes (congenital abnormalities and deaths), for decades. As we will see later, there is potential for this to change with tools like continuous glucose monitoring devices (CGMs).
A result which surprised me was the risks to women with Type 1 and Type 2 diabetes was about the same and slightly higher for neonatal death in women with Type 2 diabetes. While there appears to be a trend upwards in some of these graphs, Dr. Murphy pointed out the tending was not statistically significant.

A question I had was how this compares to the general population. Dr. Robert Lindsay, covered this with some earlier data. Assuming the risk level has remained the same for the general population, for stillbirth, women with diabetes have a risk somewhere between 2-4 times higher than the general population.
For adverse outcomes (death and congenital defects), we also see similar risk profiles for women with Type 1 and Type 2 diabetes. Literally 1 in 10 women with diabetes, who do not prepare for pregnancy, have a serious complication with their pregnancy. The good news is, with planning and preparation, this number goes down to 1 in 50 which is close to the rate for the general population.
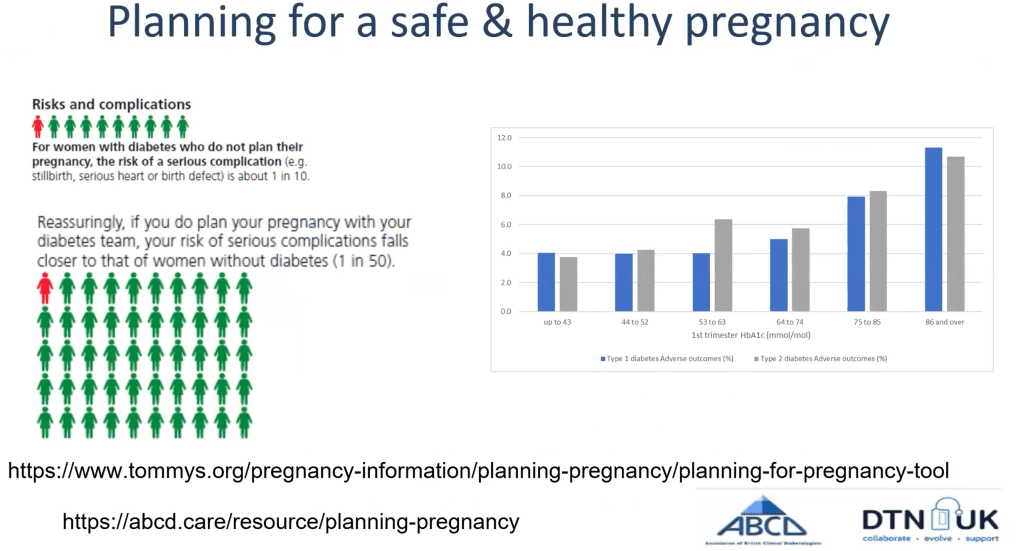
Planning and preparation in this case means taking folic acid before and during pregnancy and controlling blood sugar levels as well as possible. The guideline is to have an HbA1c below 48mmol/mol (6.5%) which, for many, is easier said than done. Many factors affect a woman’s ability to control their blood sugars beyond the usual diet and exercise. For Type 1 is was shown that other factors include:
- Age (younger Type 1s often struggle to control their average blood glucose levels compared to their older counterparts)
- Social disadvantage (Deprivation)
- Time since diagnosis (while older Type 1s typically have a lower HbA1c, those diagnosed 5 or more years ago typically have a higher HbA1c)
- BMI (the higher the body mass index, the lower likelihood of a woman with Type 1 having an HbA1c below 6.5%)
For Type 2, social disadvantage was a factor although it does not seem to be as pronounced, time signce diagnosis was a factor, and also BMI.
The only one of these factors which can be easily addressed by a woman looking to get pregnant is BMI but, as many of us know, shifting the needle on weight is not a simple task.

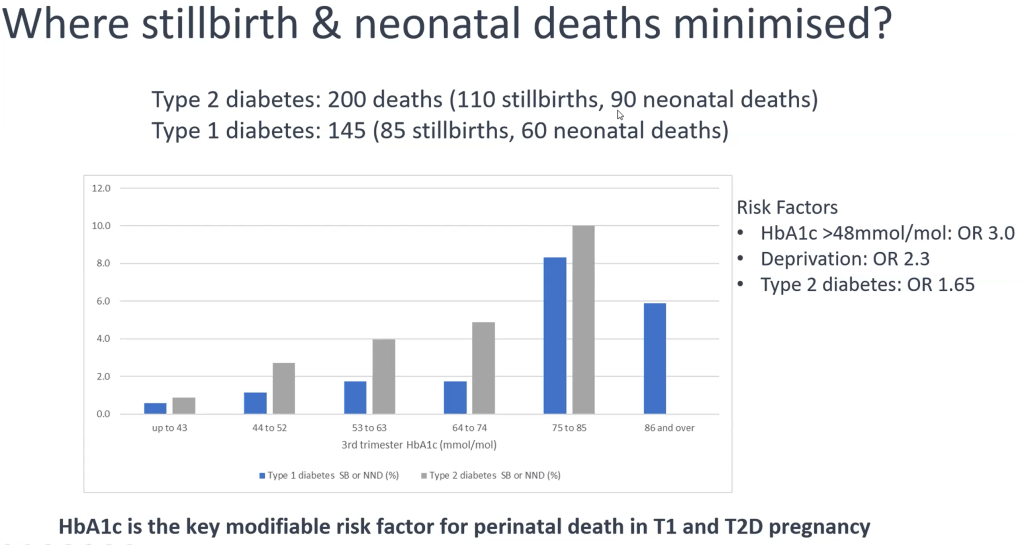
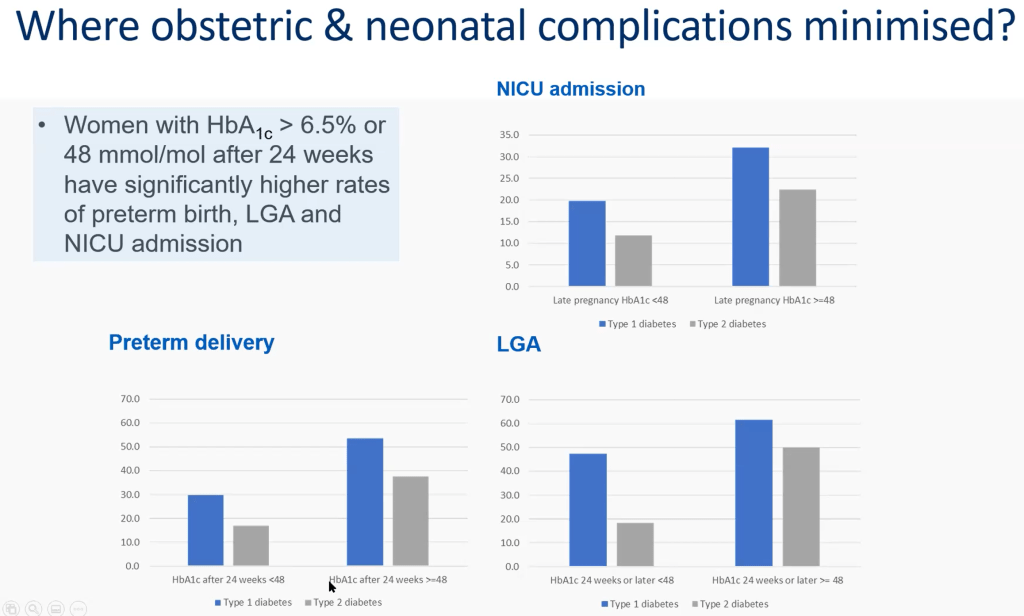
While important before getting pregnant and in the first trimester, HbA1c is also predictive of adverse outcomes as late as the third trimester. For both women with Type 1 and Type 2 diabetes, the risks significantly increase for an HbA1c above 75 mmol/mol (9.0%). Dr. Murphy also pointed out that this result removed confounders (contributing factors such as weight, age etc.) In other words, HbA1c is very predictive of risk.
She also presented details of the relative risks for Neonatal Intensive Care (NICU) admission, preterm birth, and having a “big baby” (LGA: Large for Gestational Age) showing HbA1c also predicts for these events as well.
Dr. Robert Lindsay also presented on factors associated with still birth, including those with Gestational Diabetes.
Not surprisingly, blood glucose levels are a factor here as well even for those diagnosed and treated for gestational diabetes. Given there were different results for the diagnosed and undiagnosed, it suggests there is a factor beyond fasting blood glucose affecting outcomes which treatment is addressing. My assumption is it is the non-fasting glucose levels and their fluctuations.


While the results may seem depressing, there is hope. As we will see in the next two sections, there are new technologies and treatments which can positively impact pregnancy outcomes for women with diabetes of all Types.
Health Benefits of Using a CGM During Pregnancy
Dr. Jennifer Yamamoto presented on the performance and benefits of Continuous Glucose Monitoring (CGMs) for pregnant women with diabetes.

For sensor performance, she spoke of a study looking at placement on the body of the CGM sensor covering women of all Types.

Overall, regardless of placement the accuracy as measured by MARD (Mean Absolute Relative Difference), where a lower number indicates better accuracy, performance was good but the arm was the best area for placement achieving 8.7% accuracy.

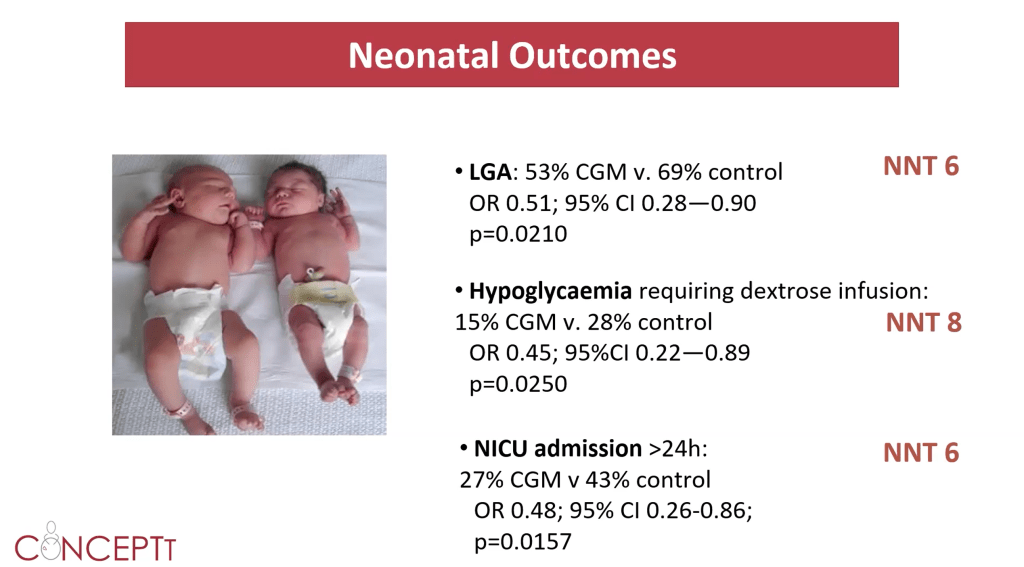
In terms of the benefit of using a CGM device, Dr Helen Murphy, presented results specific to Type 1 showing, especially in the third trimester, significantly better results for pregnant women who used a CGM; they literally gained an additional 100 minutes per day in range.

As to be expected, this had a knock-on effect on neonatal outcomes with a statistically significant lowering of risk for a larger baby (LGA), hypoglycaemia, and neonatal ICU admission.
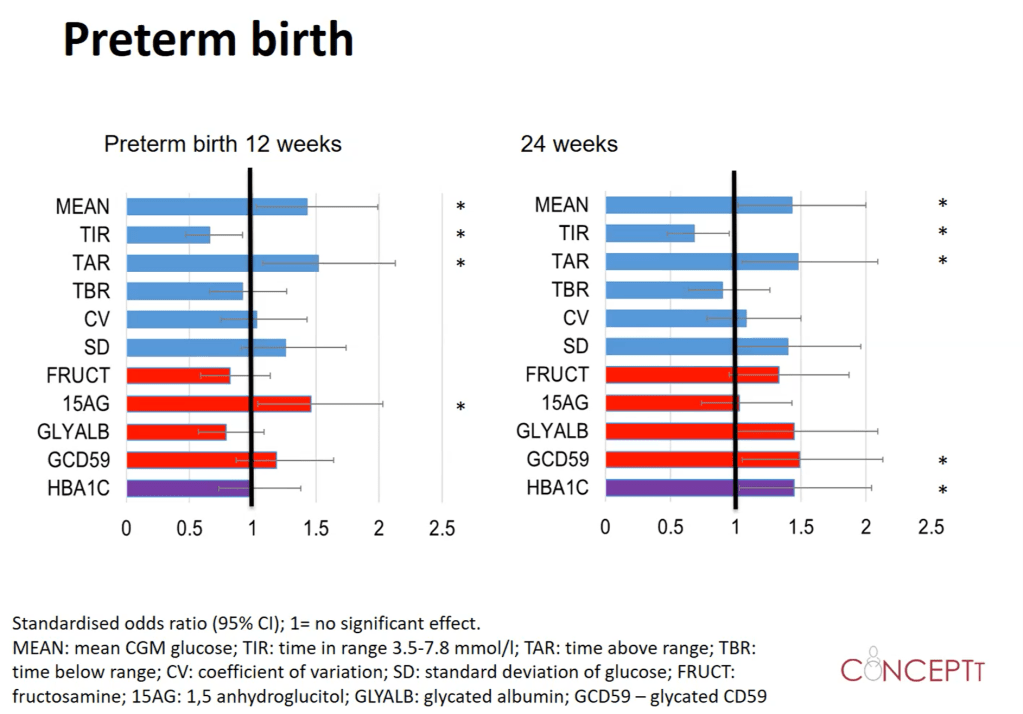
Dr. Claire Meek presented on the predictive power of CGMs for adverse outcomes, using CGM measures such as mean glucose levels (MEAN), Time in Range (TIR), Time Above Range (TAR), Time Below Range (TBR), the coefficient of variation (CV, a measure of variability of levels), and standard deviation (SD, another measure of variability). These were compared to the effectiveness of biomarkers in the blood and the traditional HbA1c.
Even for me these graphs are hard to read but the key takeaway is to look at the rows with an asterisk on the end as these are the measures which were significantly predictive. So, for preterm birth, for 12 weeks, CGM and one of the biomarkers fared well and for 24 weeks, CGM, a different biomarker, and HbA1c fared well.
Looking at predictors for a “big baby” (LGA), Neonatal ICU (NICU) admission, and Neonatal Hypoglycaemia (NH) we see CGM and HbA1c are the constant performers for prediction.


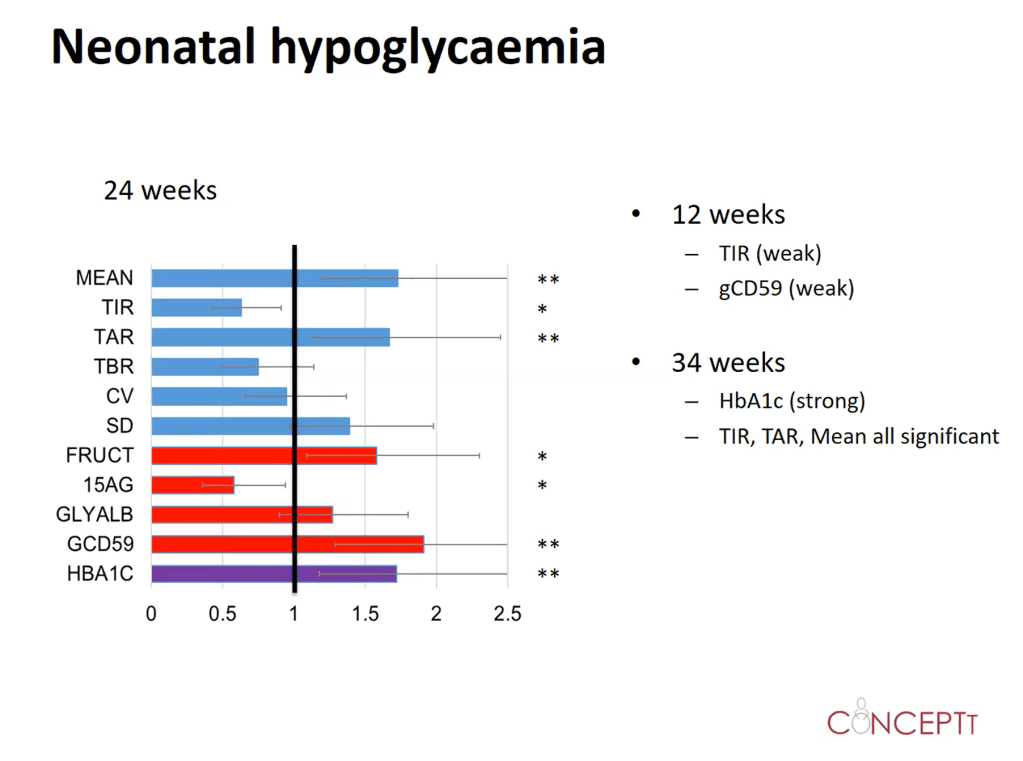
Looking at just Time in Range (TIR) and the HbA1c, we see, for early pregnancy a CGM offers good predictability and the opportunity for early intervention. Later in the pregnancy, HbA1c provides stronger predictability.

In conclusion, CGMs not only offer the ability to predict adverse outcomes early on in the pregnancy but their use can also improve them. Yet again we have compelling evidence that CGMs offer tremendous benefit to people with diabetes.
Should Women with Diabetes Take Metformin?
The final presentation I will talk about was a debate on the benefits and risks of using metformin during pregnancy. This was discussed between Professor Denice Feig who argued the “pro” case and Dr. Yariv Yogev who argued against. However, discussions in the question and answer session at the end showed both agreed on many of the key points with little debate between them.
Typically a “Type 2 drug”, metformin has many effects on the body but is broadly known as a drug which reduces insulin resistance. It is known to cross over the placenta into the baby but it is well established that it does not cause birth defects.

It is understandable that the issue of metformin use needs to be discussed/debated because international consensus on whether metformin or insulin should be used as a first line treatment is still mixed.

Professor Feig presented a meta-analysis study showing the benefit of metformin over insulin although it was clear in the discussion that many women with diabetes often used insulin as well as metformin to help control blood glucose levels.
Factors of potential concern were a lower gestational age i.e. babies were born slightly earlier and a slightly higher incidence of “small babies” or what is referred to as SGA (Small for Gestational Age).

Professor Feig presented other studies comparing metformin to insulin with similar results finding:
- Metformin helped with glucose levels after meals
- There were less cases of hypoglycaemia with metformin
- Metformin reduced the amount of weight gain in mothers and the need for c-sections
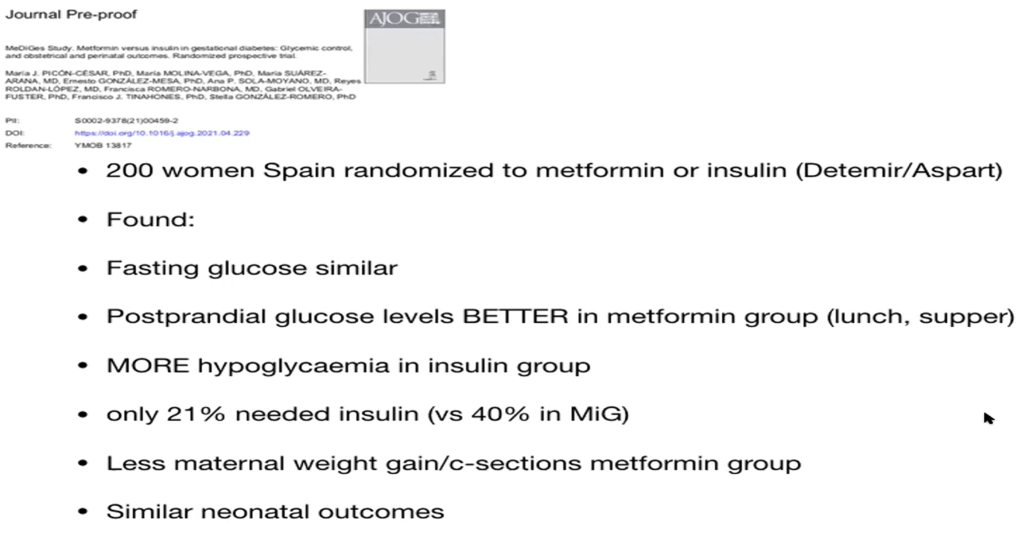
For women with Type 2 we, again, saw similar results and the potential for a “small baby”.


There was discussion on the long term effects on the baby of exposure to metformin but both presenters agreed the results are mixed and no strong conclusions can yet be drawn that there are detrimental effects.
Dr. Yogev presented a great table showing how metformin compared to a placebo for outcomes (a p-value of 0.05 or less indicates statistical significance) indicating:
- Lower birthweights with metformin
- Reduction in the rate of extremely large babies
- Increase in small babies
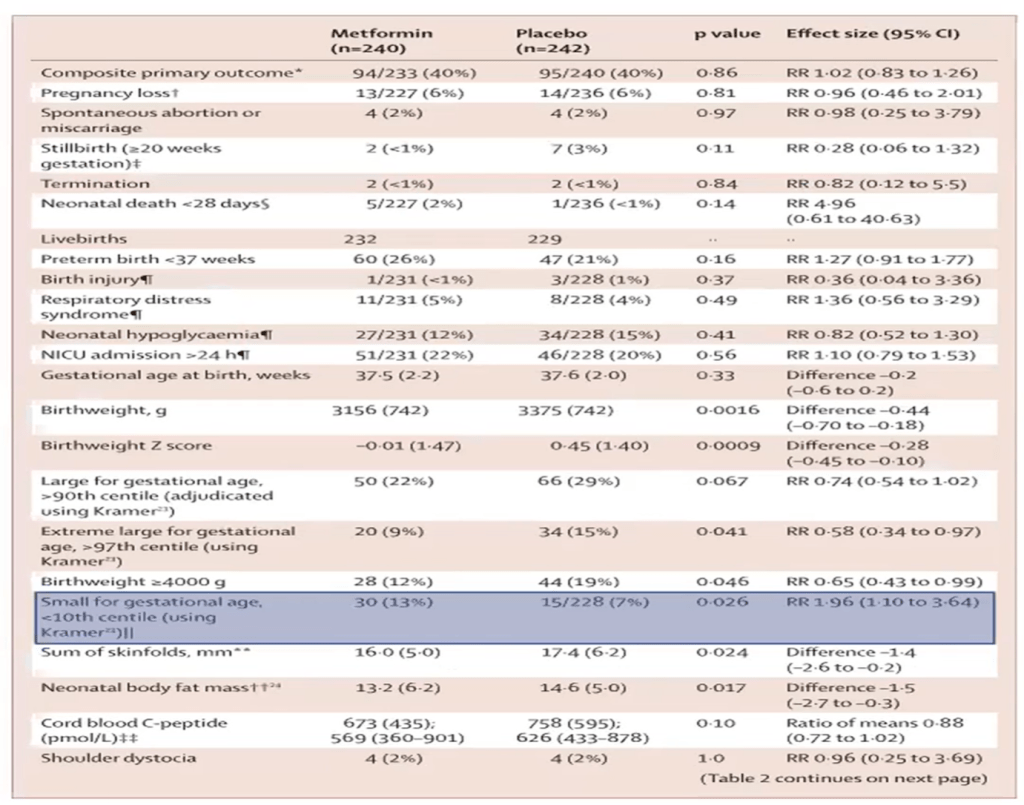
Dr. Yogev did point out that in his own studies he could not confirm the increased risk of small babies as a result of using metformin. Both agreed that where there was a risk of babies being born small, metformin may not be advisable e.g. in the case of twins. Professor Feig also made the point that, if a pregnant woman with diabetes was taking metformin and there was indications that her baby was undersized, metformin could be stopped during pregnancy to minimise any problems.
TL;DR
Health risks to the baby for women with diabetes are:
- Higher risk of stillbirth and neonatal death (death in the first few weeks of birth) compared to the general population
- Higher risk of congenital defects
These risks can be reduced through taking folic acid both before and during pregnancy and reducing HbA1c. However many factors affect the ability to reduce HbA1c such as age, social disadvantage, time since diagnosis, and weight. While difficult, HbA1c is a strong predictor of outcomes at all stages of pregnancy so any intervention which can help reduce HbA1c is of significant interest.
One intervention which shows promise are CGMs whose measures are predictive of outcomes (especially in early pregnancy while HbA1c is good at predicting outcomes later in pregnancy) and, therefore CGMs can be used to advise early intervention. It was also shown that the use of CGMs for women of all Types saw a reduction in adverse outcome risk. For pregnant women using a CGM while accuracy was good wherever the sensor was placed, placement on the arm showed the most accurate results.
A second intervention which shows promise is metformin, a drug which lowers insulin resistance. While reducing risk across most measures, there was potentially an increased risk in a smaller baby for gestational age (SGA). It was agreed that, in most cases, the risk could be managed through active monitoring of the pregnancy (and taking the pregnant woman off metformin if needed) but for cases where there was an existing known risk of SGA (twin birth, for example) metformin would not be advised.