I have written before about taking insulin through customs but, with a trip to the US happening tomorrow and a trip to Germany completed two months ago, I thought I would pass some thoughts on about travelling as a pumping and CGMing type 1. This is part one (Day Pack) with part two (interstate and overseas travel) coming after my trip and with the wisdom gained.
The Spreadsheet
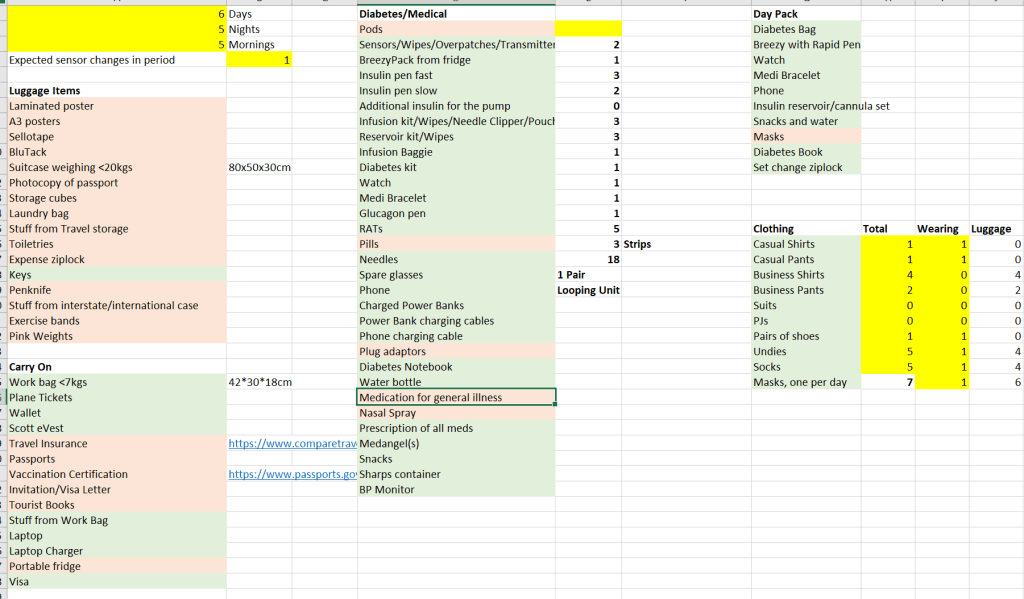
This spreadsheet removes a lot of the thinking when it comes to packing. The Day Pack list is in the top right.
Day Pack
My Diabetes Bag

My Day Pack is the conference bag from the Berlin trip. I also use this as a bag for all my carry on medical supplies when travelling interstate or overseas. Why a bag just for medical supplies? Because most airlines these days do not count medical supplies towards carry on quotas so it is easier to show them what is being excluded if it is all together. For the local Jetstar airline, who weigh carry-on luggage, this makes the process slightly less excruciating. The bag is also easy to locate when I need to do a set change mid-flight. This also means less bag swaps whenever I travel for the day/interstate/overseas as the core set of stuff in this bag never change.
Here are the contents of the bag:

Going from the top we have:
- Diabetes kit with finger pricker, glucose tabs, lip balm, Splenda tabs, lancets, batteries, prescriptions, business cards of my health care team, and blood/organ donor cards
- A USB fridge (a new addition yet to be tested in the wild)
- Spare prescription glasses
- N95 mask
- Tissues
- Sharps container (for those mid-flight set changes etc.)
- Hayfever/cold nasal spray
- BreezyPack with MedAngel inside (NB: I could not find a reliable link for buying MedAngels but it is a great Bluetooth temperature monitor)
- Glucagon pen
- Needles for emergency
- COVID testing kit (just in case)
- Hypo snacks
- Power banks and cables (when you rely on technology to keep you alive 24-7, you want backup power sources and the ability to charge devices)
- A spare pump
- A transparent packing cube for needles and insulin so it can be easily pulled out at security
FlexPen(s)
I use Novorapid FlexPens cartridges to refill my pump and this also means I have the FlexPens on hand if the pump has a catastrophic failure so, for day trips, I carry 1-2 NovoRapid pens in the BreezyPack in case I need a refill or if I need to fall back to multiple daily injections.
Diabetes-Compatible Watch
My watch is a cheap TicWatch but, with xDrip+ as a companion app to CamAPS FX, I get access to my CGM data and have it appear on my watch. Very useful when you want to quickly check your BGLs but you are in a tiny economy class seat and your phone is in your pocket or when you are in a business meeting and it might be considered a step too far to pull out the phone and start swiping.

Medi/Emergency bracelet
A medi/emergency bracelet is a must for me, especially if I am travelling solo.
Mobile Phone
Being the brain of my CamAPS looping application, my phone comes with me everywhere.
Pump Consumables
In terms of pump consumables, for day trips, I generally carry a spare infusion set and cartridge set in case I am caught unawares while out and about. In a pinch, I can make a full set change without drama.
While I could also carry a spare CGM sensor, the applicator for the Dexcom G6 is so large, I generally do not bother as, at worse, it will mean a few hours with looping off and no CGM data (for the pump the default basal settings will take over and, for me, they are well tuned so it will keep me going until I get home.) I also have the finger pricker in the diabetes kit if I want to double-check.
Snacks and Water
While my bag has snacks inside for hypos, this entry is a good reminder to put in a water bottle and check expiry dates.
Masks
Not strictly needed for diabetes management but good to carry in case you go to crowded places with people coughing or if you are travelling and mask wearing is required. I generally carry N95 or equivalents and, as mentioned above, normally have a spare in the bag.
Diabetes Book
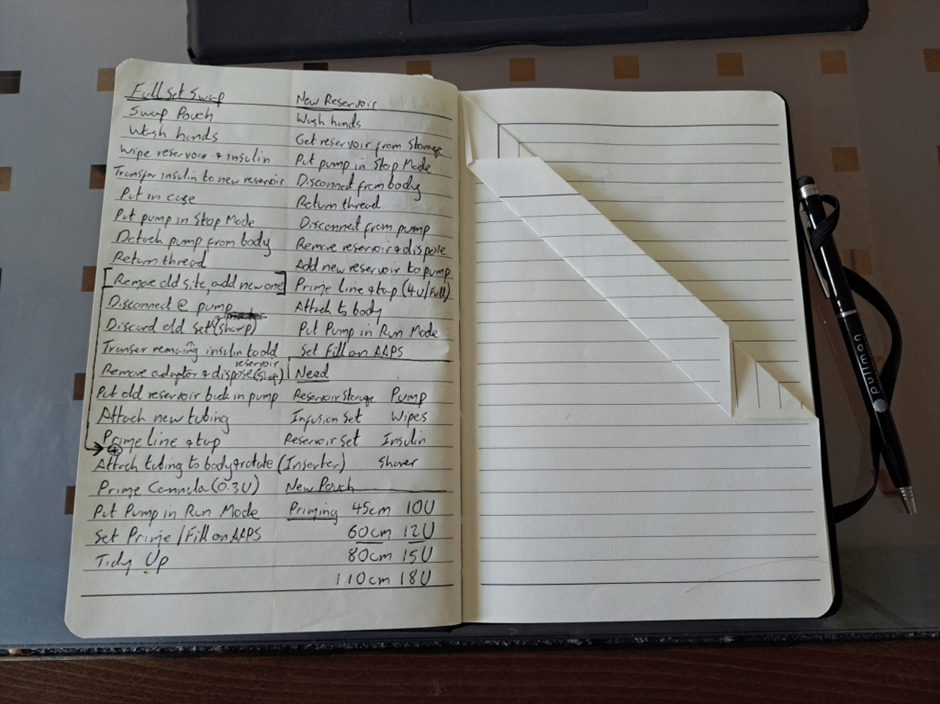
This contains a wealth of information including, as can be seen above, step-by-step instructions for essential tasks like set changes and cartridge swaps. Some of the veteran type 1 folk laugh at the fact I rely on a book for, what is to them, second nature but, frankly, if I am jetlagged, half-asleep, half-drunk, and/or in some other compromised state, I would much prefer to trust the book than my foggy head.
Other information it contains are my profile settings, an on-going list of foods I discover I can snack on without spikes, support numbers for equipment, and miscellaneous diabetes thoughts or ideas jotted down on the run.
Set Change Ziplock
This is a bag of “stuff” I need to do set changes (cartridges and infusion sets). This does not sit permanently in the diabetes bag as I use it all the time.

We have:
- Emergency antiseptic gel (in case I run out of wipes)
- Ypso cartridge box (which I also use to store the Ypso coin, batteries, and other Ypso-related set change stuff)
- Ypso cannula inserter
- Safety razor (for shaving a spot for the cannula to go)
- Jar grips for pulling FlexPens apart to get to the insulin
Conclusions
That is my current kit. It does evolve over time but is relatively stable at the moment. If you have other items you carry with you on day trips, feel free to add a comment.