This week I underwent an experiment to see what would happen if I combined a very low carbohydrate meal replacement, a commercial looping system, and snacking to cover hunger pangs. The results were better than I expected and, over the four days, I was seeing normal, non-diabetic blood sugars. Unlike other regimens, I did it with:
- No exercise
- No bolusing
- No hypo treatments
- No meal plans
- With insulin resistance and a daily insulin requirement of over 70 units per day
You can see the details of the setup here but, in this post, I thought I would go through the results and, now I am on the other side, reiterate why I believe it is a superior approach to Dr. Bernstein’s.
Before and After
So, before the four days, I had:
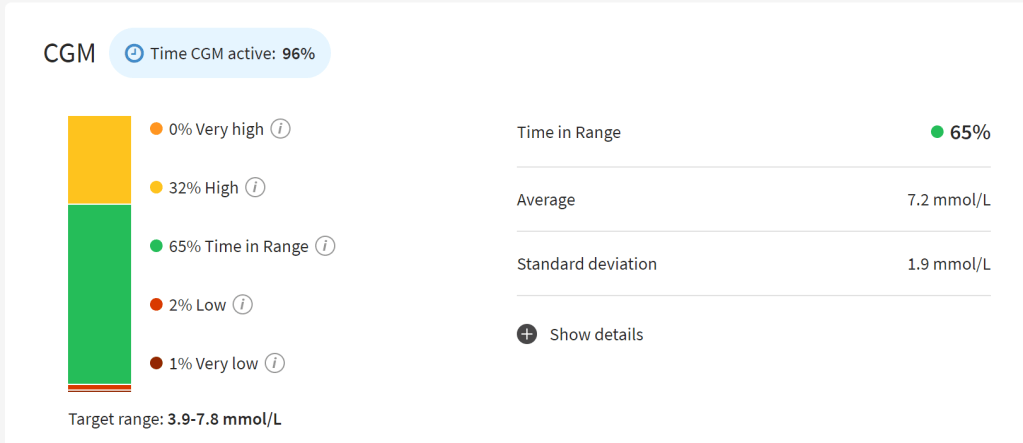
- Average Glucose of 7.2 mmol/L (130mg/dL) (over 14 days)
- Average Glucose of 6.5 mmol/L (117mg/dL) (over 2 days)
- Standard Deviation 1.9 mmol/L (34 mg/dL) (over 14 days)
- Standard Deviation 2.3 mmol/L (42 mg/dL) (over 2 days)
- Median 6.2 mmol/L (112 mg/dL) (over 24 hours)
- Coefficient of Variation 35% of Mean (over 2 days)
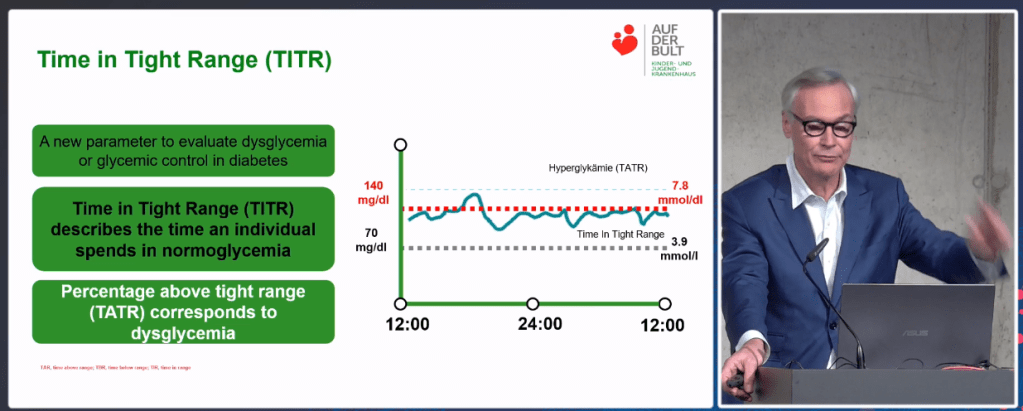
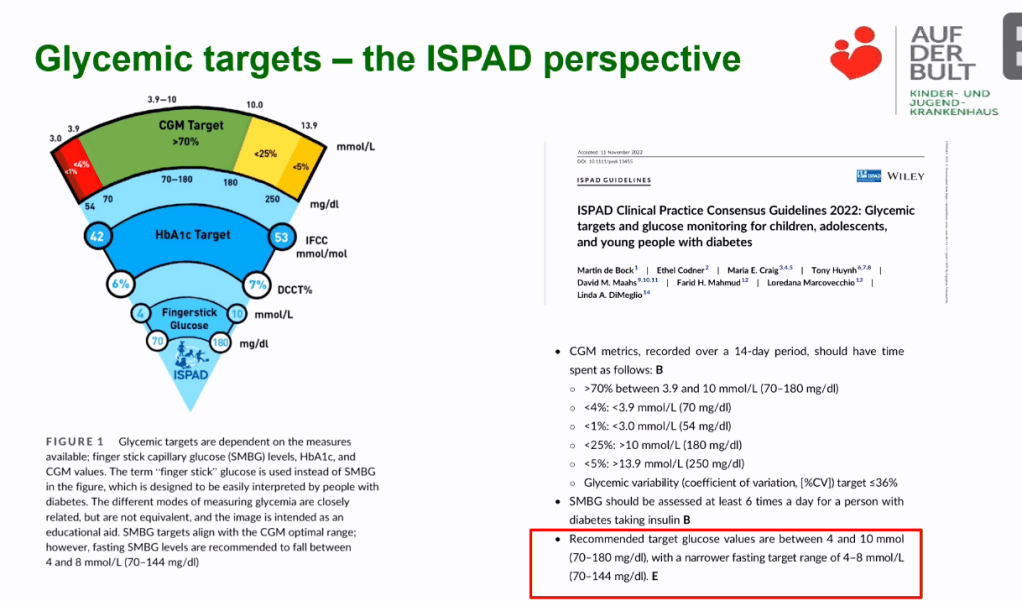
- Time in Tight Range (3.9 – 7.8 mmol/L aka 70 – 140 mg/dL): 65%
- Highs: 7 Lows: 11 (over 2 days)
- GMI of 6.1% (over 2 days)
Let us now look at the results at the end of each day (screenshots taken just after midnight each night)
Day 1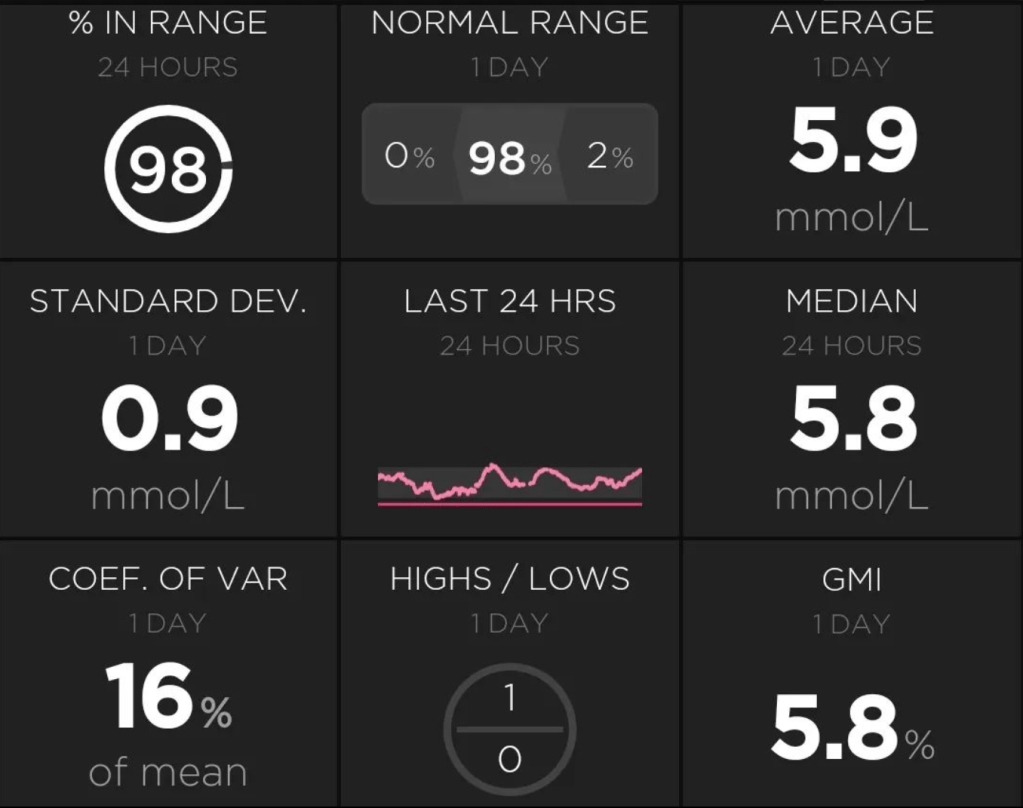 | Day 2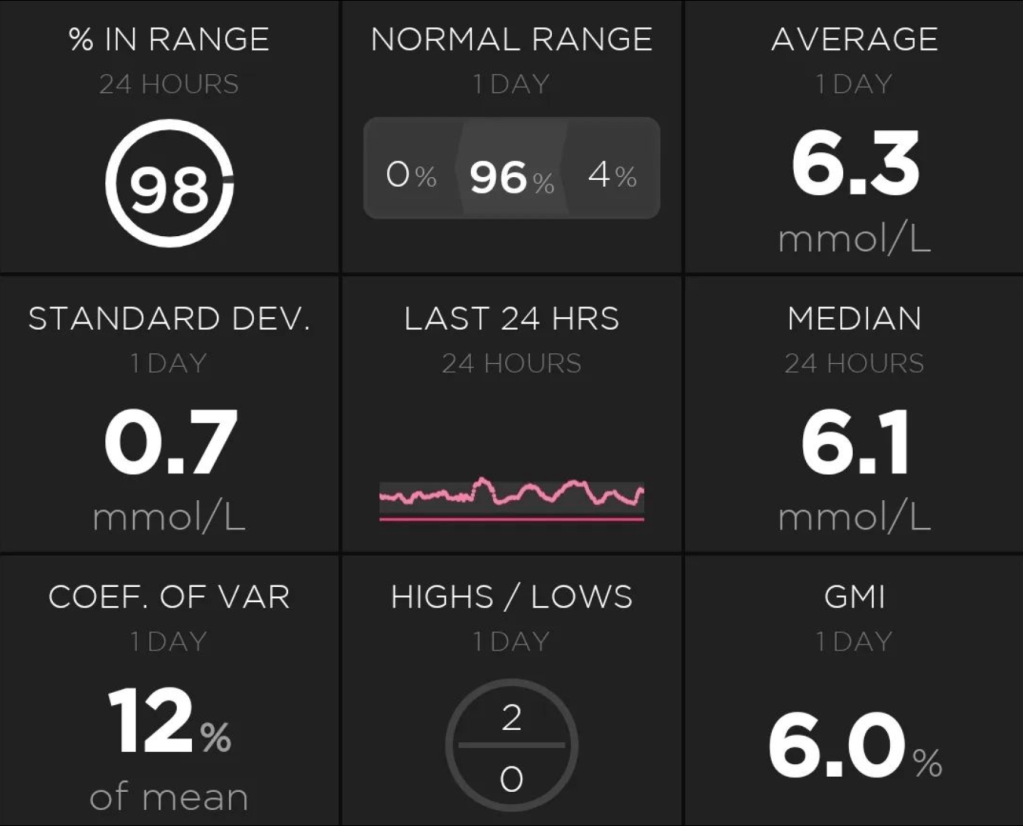 |
Day 3 | Day 4 |
For the totals above, as can be read with a keen eye, all graphs are for 24 hours. The range is the Time in Tight Range (TITR) (3.9 – 7.8 mmol/L aka 70 – 140 mg/dL).
Comparing we see every measure (except the Median, especially on Day 3) has significantly improved. Highlights include:
- Halving the Standard Deviation and Coefficient of Variation.
- Taking my TITR from the mid-60s to the high 90s
- Eliminating my lows (although I suspect they were calibration errors from a new sensor) and significantly reducing my highs (these were real).
For completeness, my weight stayed about the same, and my daily insulin requirement stayed about the same (84-79 units) as well. This second result genuinely surprised me as I assumed the sudden drop in dietary carbohydrate would lead to a much lower insulin need. I assume the difference in carb was offset by the increased protein and further amplified by the increased consumption of animal fats, raising my insulin resistance.
Did You Really Achieve Normal Blood Sugars?
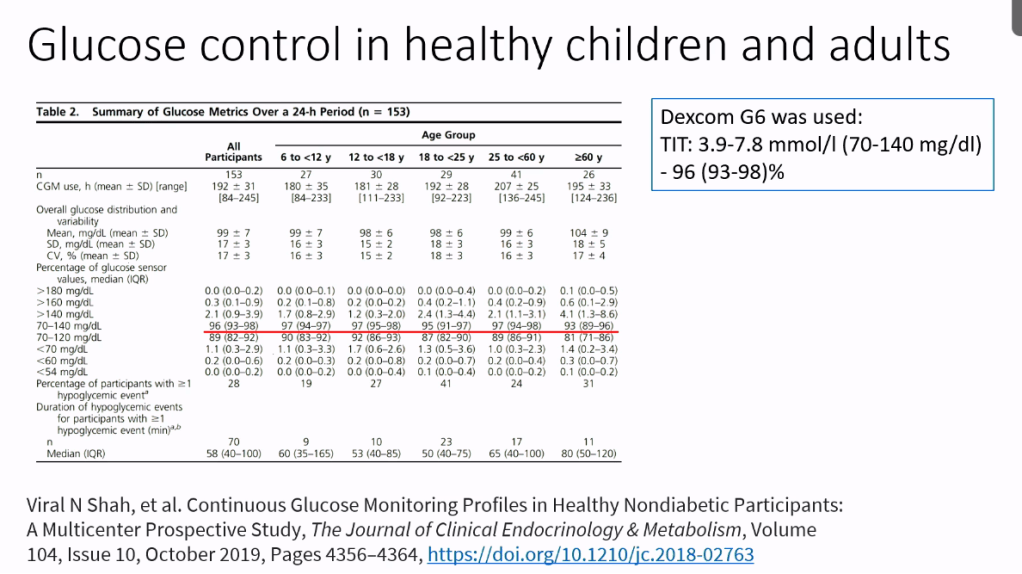
Let us consider a study of the blood sugars of non-diabetics I mentioned in another recent post.

Lots of numbers here, so let me translate the key points for the average participant:
- They had a mean value of 99 +/- 7 mg/dL (5.5 +/- 0.4 mmol/L)
- Their standard deviation was 17 +/- 3 mg/dL (0.9 +/- 0.2 mmol/L)
- Coefficient of Variation was 17 +/- 3 %
- TITR was 93-98 %
- Time in Super Tight Range (TISTR) (70 – 120 mg/dL aka 3.9 – 6.7 mmol/L) was 82-92%
- Time below range was about 1.3% of the time
I only measured TISTR once during the four days which looked like this:

Where I measured 92% TISTR, beating the non-diabetic value of 90% and hit every range on the non-diabetic normal blood ranges.
The only measure I did not consistently hit was Mean Glucose on days two and three due to my morning coffee throwing out my values. By day four I had adjusted the coffee not to spike me so I think it is fair to say that, with improved experience managing the snacks and setting my pump to a more aggressive target (it was set to 5.4 mmol/L aka 98 mg/dL for the experiment but can be set as low as 4.4 mmol/L aka 80 mg/dL), given I had zero lows during the four days, it would not be hard to consistently hit this range as well.
Why Do You Say It Is Superior To Dr. Bernstein’s Approach?
In terms of the results I expect it is possible to get similar results with Bernstein but where I see this approach having the edge is:
- Food management is MUCH simpler: Aussielent takes care of the main meals and you simply choose snacks which you like and which work for you. Compare this to Bernstein where you have to craft meal plans (he literally wrote a nearly 300-page book just on this topic alone), have no snacking, have to consider “forbidden” and “allowed” foods; it is a lot more work
- Insulin management is MUCH simpler: Getting the looping pump to do the heavy lifting means I literally go for hours a day, not thinking about diabetes and I never need to “sugar surf” my way down. For the above results I did not even declare carbs or bolus; the loop took care of it. In the case of Bernstein, from Dave Dikeman’s video which I mentioned in my preparation blog, we learn he treats lows with glucose 1-2 times a day and, if he goes above 110 mg/dL (6.1 mmol/L) he uses an intramuscular shot of rapid acting Novolog. This is not including any R-insulin injections he does to cover meals, plus injections for basal and dawn phenomenon management.
- Hormone fluctuation management is MUCH simpler. A good example of this is dawn phenomenon. For someone who is looping, the pump manages it overnight with no human intervention required. Here, Dr. Bernstein admits he and most of his Type 1 patients go up overnight and his solution is getting up, every night around 4am and doing multiple injections of different insulins which, to me, is a recipe for disaster.
The fact is the most recent edition of Dr. Bernstein’s book was written over ten years ago and a LOT has changed since then. It make sense the innovations which have come over the last decade, such as looping systems, can help us manage diabetes better and remove some of the mental burden of managing the disease.
The other big advantage of the Practical Diabetic Solution is there are still plenty of levers to pull for even better results e.g. the inclusion of exercise, bolusing and declaring if required, flexibility in snack strictness to suit the individual, augmentation of pump delivery with needle delivery etc. whereas, with Bernstein, it is so strict, there is, in my opinion, little room to move or to be creative.
Will I Be Continuing The Practical Diabetic Solution?
My position has not changed. To explain my position, I will again quote Dr. Bernstein adherent, Dave Dikeman: “I want to be normal…Not normal in that I can eat a birthday cake with everybody else but normal in that I want to have the same blood sugars as everyone else”. I respect this position but I simply do not share it. I see no reason why I cannot have a small slice of cake at the occasional birthday party, estimate the bolus and have the loop soak up the rest and my Solution allows for that. My goal is to minimise maintenance and maintain blood sugars enough to minimise the risk of complications, helped by regular check-ups.
Similarly, if I go to a restaurant, I do not want to pull out a meal plan meal and eat it while my family orders; I want to share in the experience with my family and experience the food as the chef intended. Food is an integral part of human social interaction, it is even in our language; the word “companion” comes from “someone who you break bread with”, “mate” comes from “someone you share your food (meat) with”, and to nurture comes from the concept “to feed”. To shun this link is to shun who we are.
Where I am likely to embrace the Solution is at breakfast, lunch and while travelling. Morning is a rushed affair in our house so a quick meal shake which I do not need to think too hard about is perfect. As I mostly work from home, I usually eat lunch alone so, again, a shake which will not spike me and make me a zombie in the afternoon, which is perfect. Conversely, if I go into work and my colleagues go out for lunch I will join them and leave the shake in the locker. Dinner is around a dinner table and shared with the family. This is sacrosanct for us and the Solution will not be part of it.
For travelling, the Solution is perfect. At conferences or, for example, all day workshops, there is often limited eating options and the options provided are often carby. A meal replacement shake is easy to carry with me and removes the issue.
What About You?
For someone looking for some stability in their numbers and piece of mind, consider the Solution. As mentioned here, the latest clinical thinking is an HbA1c below 6.5% or a TITR of greater than 50% is sufficient to avoid the risk of long term complications. Even if you just replace breakfast, you will likely be gluco-normal through the night (thanks to the loop) and up to lunchtime, which is already more than half the day i.e. more than 50% TITR. Anything above and beyond this is a bonus.
For the person aiming for normal blood sugars, the plan, as I followed it, is worth considering and the barrier to entry and exit are quite low as it does not require exercise, food plans, and kitchen overhauls (other than waiting a few days for the Aussielent or equivalent to turn up). If, like me, family dinner is important, you can “snack” on the elements which will not spike you which they are eating, while drinking your meal replacement (which is what I did this week). I literally saw stunning results by the first day so try it and, if you do not see improvement, move on.