For the final results, go here.
Let me start by making it clear I am quite the fan of Dr. Bernstein. I have his books and have watched all of the Diabetes University videos on YouTube. If you are new to diabetes and want a foundation on the disease and how it works, his videos are a great place to begin. Dr. Bernstein took responsibility for his disease and came up with a solution which worked really well for him. He then published his method and a lot of people have success with it. However, the last version of his book published was over 10 years ago. A lot has happened in regards to technology, medications, and food options in that time so I thought it was worth exploring how to improve on his work for my own personal benefit and that of the diabetes community.
What Is Dr. Bernstein’s Diabetes Solution?
I had a quick browse through my copies of “Dr. Bernstein’s Diabetes Solution” and “The Diabetes Diet” but could not find a good summary of his approach. Diabetes Daily give some good context on the man and the solution which may be worth a read. In short, Dr. Bernstein’s goal is for people with diabetes to have “normal” blood sugars i.e. blood sugar levels indistinguishable from non-diabetics. His approach involves:
- Low Carbohydrate (less than 30g/day) and high protein/moderate fats
- Three meals per day, no/limited snacking, with each meal having effectively the same macronutrient profile each day
- His starting suggesting is a breakfast with 6g carbohydrate, lunch with 12g carbohydrate, and dinner with 12g carbohydrate
- He advocates regular exercise which promotes muscle growth, weight loss, and improves insulin sensitivity
- “Insulin Hacking” i.e. intramuscular injections using rapid insulin
- He is generally against the use of technology in his book, preferring multiple daily injections although concedes Continuous Glucose Monitors (CGMs) may have their uses (“If I were living alone, I’d use a CGM to protect from nighttime hypoglycemic episodes” – Diabetes Solution, p357). For pumps, Bernstein lists a range of advantages and problems on pages 330-332. Quotes include:
- “Corrective injections are elegantly simple” – Diabetes Solution, p331
- “Pumps can be set to automatically increase the basal delivery rate shortly before arising in the morning, thereby circumventing problems associated with the dawn phenomenon” – Diabetes Solution, p331
- “Insulin pumps cannot be used to give intramuscular injections for more rapid lowering of elevated blood sugars” – Diabetes Solution, p331
- “Contrary to a common misconception, they do not measure what your blood sugar is and correct it automatically” – Diabetes Solution, p332
- If you have the book, check them out. For me, many of the criticisms of pumps equally apply to multiple daily injections over a prolonged period but decide for yourself
To see Dr. Bernstein’s Diabetes Solution in action, Dave Dikeman is a great example. He has been living with type 1 diabetes since the age of nine (he is now around 18 years old) and has worked closely with Dr. Bernstein, (I believe assisting with his YouTube channel) for many years. He presented his approach to Low Carb Down Under about a year ago. It is a great summary of how the solution works and shows someone achieving great success with it.
What Results Can We Expect From Dr. Bernstein’s Diabetes Solution?
Fortunately, Dr. Bernstein published the results of people dedicated to his approach five years ago. Key results were:
- A survey was conducted on members of the Facebook “Typeonegrit” group with 316 respondents, a group of “type 1’s and parents who follow Dr. Bernstein”
- Average time following Dr. Bernstein’s Diabetes Solution was 2.2 ± 3.9 years
- Mean daily carbohydrate intake was 36 ± 15 g
- Average HbA1c was 5.67% ± 0.66%
- 2% of respondents reported diabetes-related hospitalizations in the past year
My Current Approach And How It Compares
Using the Bernstein summary as a prompt, here is my current approach:
- “Low-ish” carbohydrate: I do not count carbs but estimate I eat maybe 100-150g per day
- I generally have a white coffee for breakfast, nothing regular for lunch (sometimes food, sometimes snacks, sometimes nothing), and dinner with the family which usually has no more than 50g per serving, but this is not a hard rule
- Snacking happens when I want. It is small and I do not give it too much consideration
- Little to no exercise
- I use a commercial looping pump/cgm. No injections, no finger pricks
- I do not declare any carbohydrates, do not bolus or boost; the loop takes care of it
In terms of the results I am getting, I have been looping for close to 12 months and my last HbA1c was 5.5%. Given I am not following Dr. Bernstein’s Diabetes Solution at all and getting superior results to the average participant in the Typeonegrit survey, over a shorter period of time, perhaps there is value in assessing a hybrid approach for even better results.
Simplifying Food
A big part of any summary of Dr. Bernstein’s Diabetes Solution involves the listing of forbidden and allowed foods. In the Diabetes Daily summary mentioned above, of the 5,700 words, 4,500 describe which foods can and cannot be eaten. That is over 3/4 of the description. In Dr. Bernstein’s Diabetes Solution, chapters 9, 10, 11, and 25 (roughly 120 pages out of 460 pages or a quarter of the book) cover food and its management. I think it is fair to say food management is a big part of Dr. Bernstein’s Diabetes Solution.
Two years after the last version of Dr. Bernstein’s Diabetes Solution came out, a company called Soylent appeared offering nutritionally complete meal replacements for time-poor people who do not like cooking. Other companies offer similar products, including Aussielent which also offer a low carbohydrate alternative (shown below).
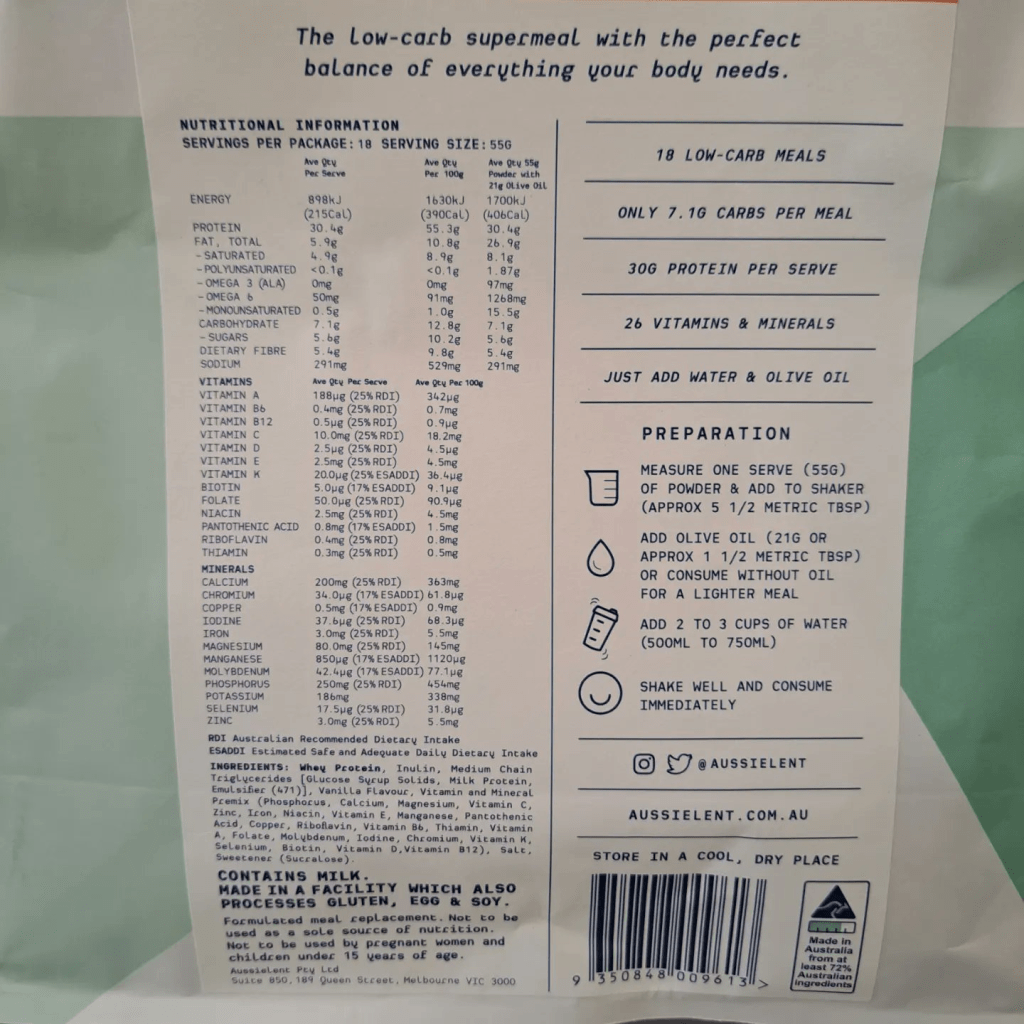
A serving provides about a quarter of the body’s micro-nutrients. For macro-nutrients a serving provides:
- 1700kJ (406 Cal)
- 30.4g Protein
- 26.9g Fat
- 7.1g Carbohydrate (excluding fibre)
- 5.4g Fibre
So, in theory, four servings a day will provide all the micro-nutrients the body needs. It passes the “less than 30g of carb per day” test of Bernstein and gives a total energy of 6,800kJ (1,624 Cal). The average adult requires between 8,700kJ – 10,500 kJ (2,000 – 2,500 Cal) per day to maintain a healthy weight (https://www.healthdirect.gov.au/kilojoules, https://www.nhs.uk/common-health-questions/food-and-diet/what-should-my-daily-intake-of-calories-be/) so we have a deficit of at least 2,100 kJ (500 Cal). Also, the packet is clear in saying “Not to be used as a sole source of nutrition”. So, we can embrace the energy deficit and lose some weight or use it for snacking. As long as the snacks do not spike us we are good to go. There are plenty of foods which, as people with diabetes, we know we can eat without spiking. For me, I will be eating things like:
- Home made protein balls (about 735 kJ/175 Cal each)
- Cheese and crackers (516 kJ/125 Cal)
- Water Chestnuts and Soy Sauce (about 190 kJ/45 Cal)
Drinks will be sugar free so it will be diet soft drinks, mineral water (soda water), sugar free cordial, and tea/coffee.
I also only have enough Aussielent for four days so this will be the length of the experiment.
Exercise
There is no doubt exercise is good for anyone. I will not be changing my routine for the next four days though. Clearly, if there was a desire to make this a long-term venture, introducing exercise would be good. Keeping this as=is also removes it as a confounding variable in the results.
Measuring and Administering Insulin
I have no doubt the use of a CGM and a Pump, with looping, have been a big part of my success to date. The pump is watching my blood sugars every five minutes and making adjustments to move my levels towards my target (currently 5.4 mmol/L or 97 mg/dL). Unlike Dr. Bernstein’s Diabetes Solution, which relies on basal insulin (sometimes delivered in the middle of the night to counter dawn phenomenon), and injecting insulin into muscles, my loop has no reliance on me being awake, or “insulin hacking”.
Looping was not available when the last edition of Dr. Bernstein’s Diabetes Solution came out which is why he says “they do not measure what your blood sugar is and correct it automatically”. Today, they can, and are very, very effective at managing overnight and hormonal fluctuations.
How Will I Measure Success?
My plan is to document my baseline in this blog and then review afterwards and see what has changed.
Current weight: 112kgs (246 lbs)
Last Daily Insulin Amount: 84 Units
Diasend (https://diasend.com/)
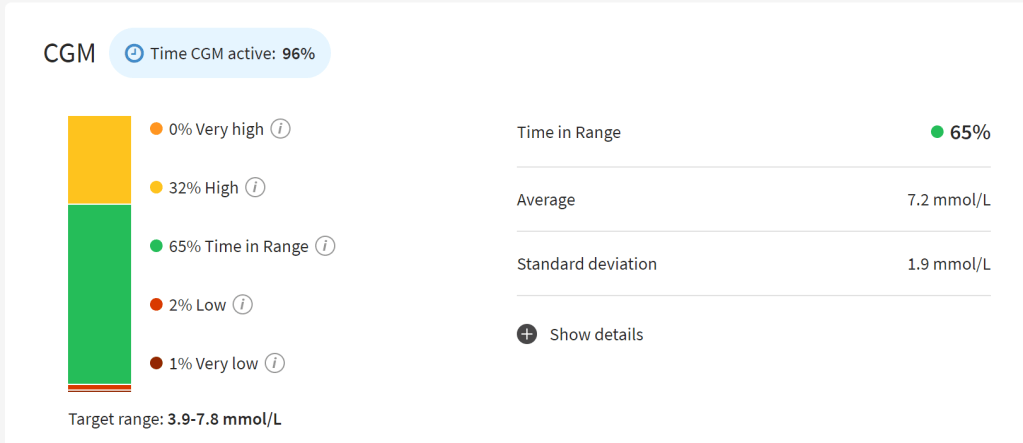
- Average glucose: 7.2 mmol/L (130 mg/dL)
- Standard Deviation 1.9 mmol/L (34 mg/dL)
- Time in Tight Range (3.9 – 7.8 mmol/L aka 70 – 140 mg/dL): 65%
Sugarmate (https://sugarmate.io/home)

- % in Range (daily TIR 3.9 – 10 mmol/L aka 70 – 180 mg/dL): 69%
- Time Below Range: 7% / Time In Range: 67% / Time Above Range 26% (TIR)
- Average 6.5 mmol/L (117 mg/dL)
- Standard Deviation 2.3 mmol/L (41 mg/dL)
- Median 6.2 mmol/L (112 mg/dL)
- Coefficient of Variation 35% of mean
- Highs: 7 Lows: 11
- GMI: 6.1%
Tidepool (https://app.tidepool.org/)
1 week values

- Time In Range (4.0 – 10.0 mmol/L aka 72 – 180 mg/dL): 88%
- Time Above Range: 9.3%
- Time Below Range: 3%
- Average Glucose: 7.2%
- Standard Deviation: 1.9 mmol/L aka 34 mg/dL
Notes:
- The lows are due to poor readings of the CGM on insertion, as confirmed by finger pricks (the only time I do them). For me, the G6 sensor reads low for the first few days after insertion
- Variation between the reports is generally due to differing periods of review. For Diasend it was the last week of data, for Sugarmate it is written on the measure (some say 2 days even though I specified 3, I am not sure why this is the case), and Tidepool was one week.
Are You Planning To Continue With This Approach?
Only so much can be demonstrated over four days. My primary reason for doing this is to see if Aussielent meals are a viable option when I am travelling for work as I have less control over what I eat when at conferences or onsite with clients. Carrying some powder and olive oil while travelling is a relatively simple solution. However, if I can also develop some preliminary data combining looping technology and a very-low carbohydrate diet, this may be worth more analysis later either by me or other people curious to try different approaches.
I actually have no interest in pursuing a very-low carbohydrate regimen long term. The primary goal of Dr. Bernstein’s Diabetes Solution is normal blood sugars. My goal is to minimise maintenance as much as possible to reduce the risk of burnout i.e. a sustainable approach, and to minimise the risk of long term complications (which is not quite the same as normal blood sugars). What I mean by this is maintaining a sufficiently low HbA1c that clinical evidence suggests I am close to the same risk of long term complications as a non-diabetic and getting regular check-ups is enough for me; I do not need to obsess about every spike or deviation.
Also, I like going out to restaurants and eating meals as the chef intended; I enjoy eating in moderation, rather than fixating on forbidden and approved foods; I enjoy spending literally hours a day not thinking about diabetes management. I see no compelling reason to change any of this.
Where To From Here?
For the next four days, I will be following the “Improved Solution” and writing about it next weekend. I will also be getting blood work done towards the end of this week as I am seeing my endocrinologist soon. This will give me additional results which I will publish later.

Type One Grit is given a courtesy nod by Dr. Bernstein as a trade-out for the producers time and effort in producing his videos. Many of his followers would strenuously object to being categorized as Gritters, having followed the good doctor long before the YouTube channel. In addition, the focus on Type One by the “Gritters” excludes the vast majority of diabetics.
LikeLike
Hi Morris,
My apologies for conflating the two groups in my ignorance. I’ll remove the reference to the term in the article immediately.
Leon
LikeLike
No apology or correction necessary. Your context is understood. T1Grit is a brand and in fact trademarked. Bernstein’s guidance benefits diabetics far more than the current standards of diabetes care, as does yours!
LikeLike
You seem to miss Dr B’s main point: Man made insulin is dangerous to you. Soooo …you should use as little as you can. Most diabetics die from heart attacks from long term insulin use. I know several tha have done this. Man made insulin is very diluted. Real insulin is very powerful which is the reason you body can maintain bs flat line 83 for 24hr/7day/365 days a year. You can eat a whole pizza and a gallon of ice cream and your bs will remain at 83 10 minutes after you eat and the same 83 3 hours later. Humans cannot handle real insulin. You cannot take 1/1000 of a unit of human insulin with a syringe. So human made insulin is diluted. I seldom test. As i know how much inulin i need for a meal or what will happen if I exercise. My body also tells me if I’m high or low. I take sleeping pills once a month. I do not fear od’ing while I sleep. I took one last night. Furthermore, I used to have lots of diabetic complications (no amputations) do to a DKA. I got my DKA from food poisoning which raised my bs and throwing up which dehydrated me. Most DKA’s get to a hospital in hour not the 3 days it took me (after I asked someone)which it took me). Most folks are dead without insulin for 24 hours. Now, 16 years later thanks to Dr B I am 80% recovered. Moral to my DKA story, If someone asks you to take them to a ER don’t wait 3 days, 4 hours, or 2 hours. JUST DO IT!!!! Also the CGM say what your bs was 10 minutes ago. It tests cell fluid. Finger sticks is real time directly from the blood.
.
LikeLike
My approach does use minimal amounts in that you’re only eating low carb powder and non-spiking snacks. If you want to minimise more you can through exercise etc.
LikeLike
I agree with u on the heart/insulin. …
that insulin is really watered down..real insulin u can be at a entire cake and your bs will will not rise at all..,
Do 3-15u/ bolus daily and 6u/basal ..
eat a daily salad..and am a long distance swimmer b/fly is my favorite..in my 70s Fly will definitely give me are heart attack …if I was a bad diabetic
sometimes just fast entire day on the basal..
also take occasionally sleeping pill big nono for t1s .
.try to keep bs under 100 …24/7
Have not lost my hypo signs as most t1s do
Been doing for years after my dka from food posining…,and taking 3 days to get to er while in a dka… and my body eating itself to make insulin…most folks die after 24 hours in a dka
I am not the Dr b police so do whatever u like
LikeLike
You really shouldn’t call this “better than B” because it is nothing in common with dr B
LikeLike
Why does something have to be in common with it to be better?
1. You can choose to low carb if you wish. The rule is a low carb powder (about 30g/day) plus non-spiking snacks (generally low carb)
2. Exercise is an option but not necessary if your only goal is normal blood sugars
3. I do not understand what this says
4. Bernstein on p109 talks about the problems of carb. counting, leading to his Law of Small Numbers. In my approach, the estimation error is managed by the looping pump. I also talk about it here (https://practicaldiabetic.com/2022/08/13/the-myth-of-carbohydrate-counting/)
5. I disagree that anything above 130 does damage. Long term elevated BGL does damage. My evidence is here (https://practicaldiabetic.com/2019/11/06/above-what-level-does-your-hba1c-fasting-glucose-and-glucose-spikes-do-damage/)
LikeLike