LADA often falls through the cracks between Type 1 and Type 2 Diabetes so wouldn’t it be wonderful if the world’s greatest minds came together and determined the best approach for managing LADA? In fact they did and published the conclusions in October this year (2020).
The paper is quite long but they provided nice flow diagrams which are easy to follow. If even that is too much for you, there is the tl;dr section at the end of this post.
Diagnosing Type 1 LADA
First of all the article talks about the phenotypical characteristics (how it presents) of LADA with this table summary:

As it states, none of these categorically define LADA. Fortunately, further on, it provides a flow diagram for a definitive diagnosis:

The test starts not with a glucose tolerance test, a ketone test, or a urine test but a blood test to look for the GADA auto-antibody. As LADA is a form of Type 1 Diabetes and, as the Types are defined by their aetiology (cause), the definitive test for LADA is for an auto-antibody associated to Type 1 Diabetes (GADA).
If the blood test comes back positive, the treatment applied is dependent on the patient’s c-peptide level. C-peptide is a ‘leftover’ product from the body’s production of insulin so the c-peptide level can be seen as a measure of the body’s insulin production.
For a c-peptide level less than or equal to 0.7 nmol/L the LADA algorithm (defined in the paper) is applied. For a c-peptide level above 0.7 nmol/L, the existing Type 2 Diabetes guidelines, established by the ADA (American Diabetes Association)/EASD (European Association for the Study of Diabetes) are used, with a c-peptide re-test every six months.
If the GADA test is negative, The patient may be Type 2 (or MODY or have pancreatitis) but, if LADA is still suspected (presumably based on the broad characteristics of the disease listed above), other auto-antibodies associated with Type 1 Diabetes should be tested for.
The Type 2 Diabetes Guidelines
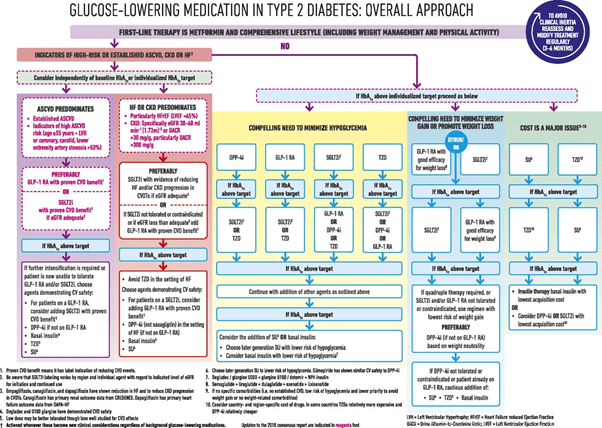
Here it is, modified in February 2020. The full paper can be found here. This is quite an involved flow diagram and, I will come back to it a little later on, in the context of LADA, but, if you are Type 2, it is worth a read to see if your health team are abreast of the latest recommendations. One point of note to LADAs who are being treated as Type 2s is the use of sulfonylureas for LADA patients is NOT recommended, whereas these drugs are often used with Type 2 Diabetics. The reason being sulfonylureas have been shown to accelerate the destruction of the beta cells in LADA/Type 1s and therefore will shorten the honeymoon before full insulin dependence.
The LADA Algorithm

Here it is. This is the flow diagram recommending the best possible treatment for people with Type 1 LADA, based on the latest information as of October 2020.
If your c-peptide level is less than 0.3 nmol/L then insulin should be used (basal and/or bolus, as required). For c-peptide levels between 0.3 and 0.7, metformin is seen as the gold standard and, as discussed in the Type 2 section above, NO sulfonylureas.
The rest of the treatments are based on the risk of cardio-vascular disease (ASCVD), heart failure (HF) and kidney disease (CKD). The flow is a little confusing but the treatments are GLP-1 Agonists (GLP-1RA): I talk about those here, SGLT2 inhibitors (these are a class of drugs which promote the passing of sugar out of the blood through the kidneys), and, if the patient’s HbA1c is above target, the inclusion of basal/bolus insulin.
How Do I Stack Up?
Being a typical LADA I thought I would run myself through the flow diagrams. While the hospital which treated my pre-diagnosis DKA failed to perform a test for GADA auto-antibodies (and simply assumed I was Type 2), my family doctor did and, on 3 March 2017, I was diagnosed as Type 1 LADA (my GADA levels were literally off the charts).
My fasting c-peptide level has never been below 1.3 nmol/L since diagnosis, so I fall under the Type 2 ADA/EASD guidelines (but no sulfonylureas!) Recommended treatments include:
- Metformin
- Weight management
- Exercise
- GLP-1RAs
- SGLT2 inhibitors
- TZDs (an insulin sensitizer similar to Metformin)
I am broadly following this recommended treatment. I use Metformin and a GLP-1RA (Ozempic/Semaglutide). I am working on reducing my weight (I fall into the ‘obese’ category for BMI) and I probably should do more exercise.
Recognizing Type 1 LADA
Based on the above recommendations, it is clear drugs such as GLP-1RAs and SGLT2 inhibitors are appropriate treatments for Type 1 LADAs with sufficiently high c-peptide levels. Yet, if we look at this Australian Pharmaceutical Benefit Scheme Press Release we see Ozempic (Semaglutide) (a GLP-1RA) is approved only for Type 2 Diabetes. The other GLP-1RA available in Australia, Trulicity (Dulaglutide), is also only approved for Type 2 Diabetes. The consequence is, instead of paying $41 a month for this recommended medicine, LADAs such as myself pay $140 per month. The $1,700 per year cost talked about in the PBS press releases is the reality for Type 1 LADAs in Australia. Moreover, while there are “Safety Nets” for PBS approved medicines, for a LADA like myself who is obtaining the recommended treatment under a “private prescription”, no safety net applies.
While having to constantly explain that insulin independent Type 1 Diabetes is a reality to medical professionals or on social media is frustrating, the significant financial impact of ignoring LADA means there are Type 1 LADAs here in Australia (and in other countries which naively consider medications as strictly “Type 1” or “Type 2”) who are not getting the appropriate treatment for their disease and this is having a direct impact on their quality of life and their ability to contribute fully to society.
tl;dr
The definitive test for Type 1 LADA is a blood test for auto-antibodies. The most common auto-antibody is GADA but, if this is negative and LADA is still suspected, other auto-antibodies associated with Diabetes should be tested for.
Once LADA is established, the treatment depends on the c-peptide level of the patient. If the c-peptide level is below 0.3 nmol/L, the patient should use basal/bolus insulin, as needed. For c-peptide levels above this, recommended treatments include:
- Metformin
- Weight management
- Exercise
- GLP-1RAs
- SGLT2 inhibitors
- TZDs (an insulin sensitizer similar to Metformin)
Sulfonylureas are NEVER recommended for Type 1 LADAs.
Sadly, in many countries, some of these treatments, such as GLP-1RAs are not recognized as appropriate for Type 1 Diabetics, including LADAs, and, therefore, are often not covered through government subsidy schemes or health insurance. If this is the situation where you live, and you are a LADA who cannot access the medications for your disease, I strongly encourage you to petition the appropriate bodies to get the guidelines changed.
