David Burren recently put me on to Breezy Packs which, if their claims are to be believed, offer a new way to keep insulin cool in the field. I have ordered a couple of Breezy Packs to put them through their paces but, first, I thought I would try out the existing methods commonly employed to show how they work.
Gel
Gel packs contain gel (no surprise there) which holds its temperature well and acts as an insulator. There is no actual cooling mechanism here other than the gel slows heat passing from one side to the other. So, to use a gel pack, you cool it down in the fridge (not the freezer as insulin does not like to be frozen) and put your insulin inside it to protect it from outside fluctuations in temperature. Outside heat is slow to heat up the gel pack which means the insulin stays cold.
Frio
Frio is, arguably, the most popular brand name for evaporative cooling pouches for keeping insulin cool. There are other brands out there (I even sell a version in my Etsy store) so feel free to shop around. They all work in the same way though. You immerse the pouch in water for, say, five minutes and it puffs up. You take it out of the water, wipe it down and put your insulin inside.
Not only are the pouch contents (generally silica gel beads or similar) an insulator but they are spectacular at absorbing and holding on to water. How Frio bags work is, when exposed to a warm temperature, the water in the beads begins to evaporate but evaporating water molecules takes energy so, instead of the external heat being used to raise the temperature of the water, some of it is used to turn the water to steam. This means the water temperature stays reasonably stable and, in turn, so does the temperature of the insulin inside the pouch. Our bodies use the same trick to stay cool when we sweat.
Breezy Packs
Breezy Packs offer a new way to keep insulin cool, which is similar to Frio bags but, instead of absorbing energy, turning water from liquid to a gas, it converts its active material from a solid to a liquid. No need to soak and wipe down. The physics of Breezy Packs is actually very smart so I will save it for when the pouches arrive and I will write another blog on the subject.
The Cooling Battleground: My Oven
It turns out that I can get my fan-forced oven down to around 30-40 degrees Celsius (104 degrees Fahrenheit) so this was my “controlled environment”. The contestants were a small Frio pouch capable of holding two insulin pens and a massive pillow gel insert.

The insert is 30x40cm with three panels. Both pouches went onto an oven tray with baking paper underneath to try and insulate from the metal bottom.

The gel pad was folded into three with two of the panels at the bottom and both pouches had a temperature probe put in the middle of them. As indicated above, the gel pad had been stored in the fridge whereas the Frio was soaked in tap water.
Once in the oven, I monitored their temperature and the temperature of the oven.
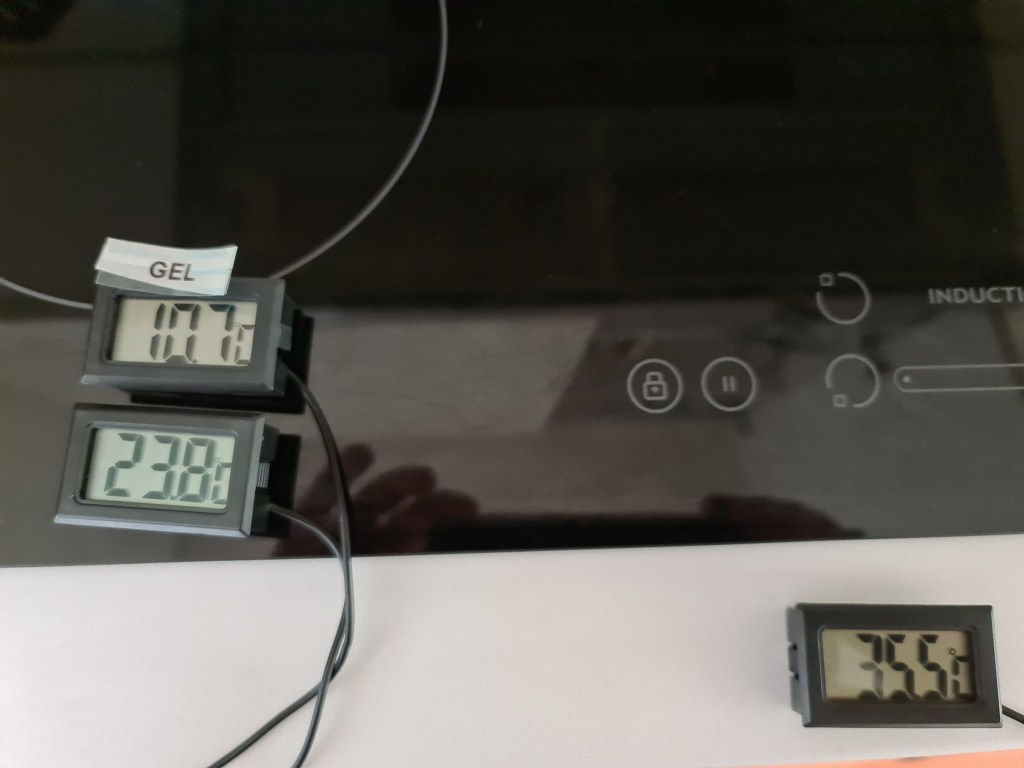
Here the gel pack is 10.7 degrees Celsius, the Frio pouch is 23.8 degrees Celsius, and the oven is 35.5 degrees celsius.
The Results
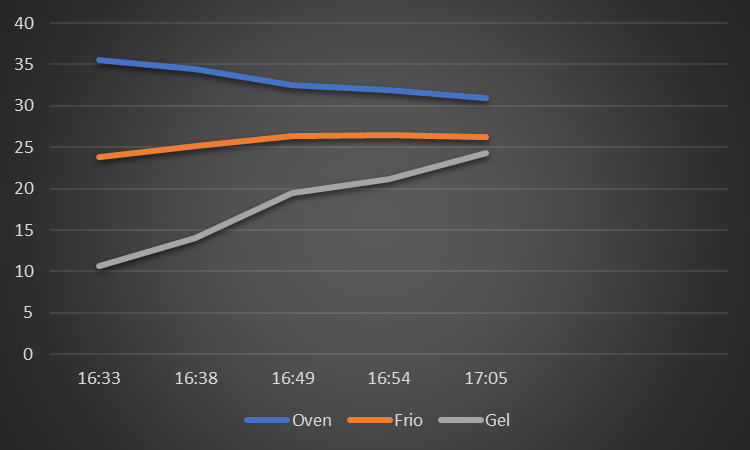
Thanks to the magic of Excel we can see how the two pouches fared. The oven temperature, which had previously reached the target temperature, was slowly dropping but remained above 30 degrees for the whole time. The Frio pouch, with the oven’s heat being used to turn the Frio’s water to steam, was holding a reasonably even temperature. The gel pouch, with nothing but insulation, slowly increased in temperature, catching up to the Frio after about 30 minutes, despite the 15 degree head start.
To be honest I was not sure the Frio pouch would work as well as it did as the oven was closed and, therefore, once the air inside the oven was saturated with moisture, the Frio would no longer be able to cool but for the 30 minutes it continued to work.
Conclusions
First of all I was really impressed the results came out as well as they did, showing the characteristics of the two pouches. For my money, if I was expecting to carry insulin for an extended period of time in high heat, I would likely look to a pouch that uses evaporative cooling. I would also invest in a MedAngel so I could check the temperature inside the pouch at any time and be alerted if things were going astray. Gel is a much cheaper option, of course, so, for short excursions, it will work fine. You could also, if you had a large enough pouch, put a cooled gel pouch inside a Frio pouch and gain a double benefit. As long as the Frio pouch is on the outside this should work fine.