Thanks to the generosity of #dedoc°, I recently had the privilege of virtually attending the world’s largest Diabetes conference: EASD 2021. Arguably the biggest news at the conference was an international consensus on the diagnosis, treatment, and management of Type 1 Diabetes. This is a comprehensive guide, backed by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD), which should, in my opinion, be the bible for health care professionals and for guiding health-related government policy.
Interestingly, last year an international consensus was released for the diagnosis, treatment, and management of LADA. I wrote a blog on it at the time going through the details. While not the same authors, nor directly endorsed by ADA/EASD, one would hope the two reports are broadly aligned in their approach given LADA is usually considered a sub-group of Type 1. In fact they are but there are differences at the edges and I raised this during the conference.

Rather than wait for the academics I thought I would go through the reports and see if I could make some headway. I will split this up into at least two parts with this one covering the diagnosis of Type 1 and of LADA.
As usual, there is the tl;dr section at the end for those that want to cut to the chase.
Diagnosing LADA
The first problem is there is no simple categorical feature of LADA. At diagnosis it shares features with “classic” Type 1 and Type 2.

So, while we can make a good guess at diagnosis, there is room for error. The report goes on to weigh up the various factors which can be used for assessment and comes up with the following flow chart.

So, first we test for the auto-antibody GADA. If it is positive, the person has Type 1 (LADA) diabetes and their treatment is then determined by their C-peptide levels. The report is vague on whether the C-peptide test is fasting, random time, or post-prandial (after a meal).
If the GADA screening is negative, the report suggests it is likely the patient has Type 2 diabetes and, therefore not LADA (although Type 3c and MODY should be considered). However, if LADA is still suspected, other auto-antibodies such as IA-2A, ICA, and ZnT8A can be screened. If these are positive, we are back to a positive diagnosis of Type 1 with treatment being defined by C-peptide levels.
Diagnosing Type 1
The Type 1 report also weighs up the various factors in diagnosing Type 1 compared to other Types, such as Type 2 and MODY and comes up with this flow chart.
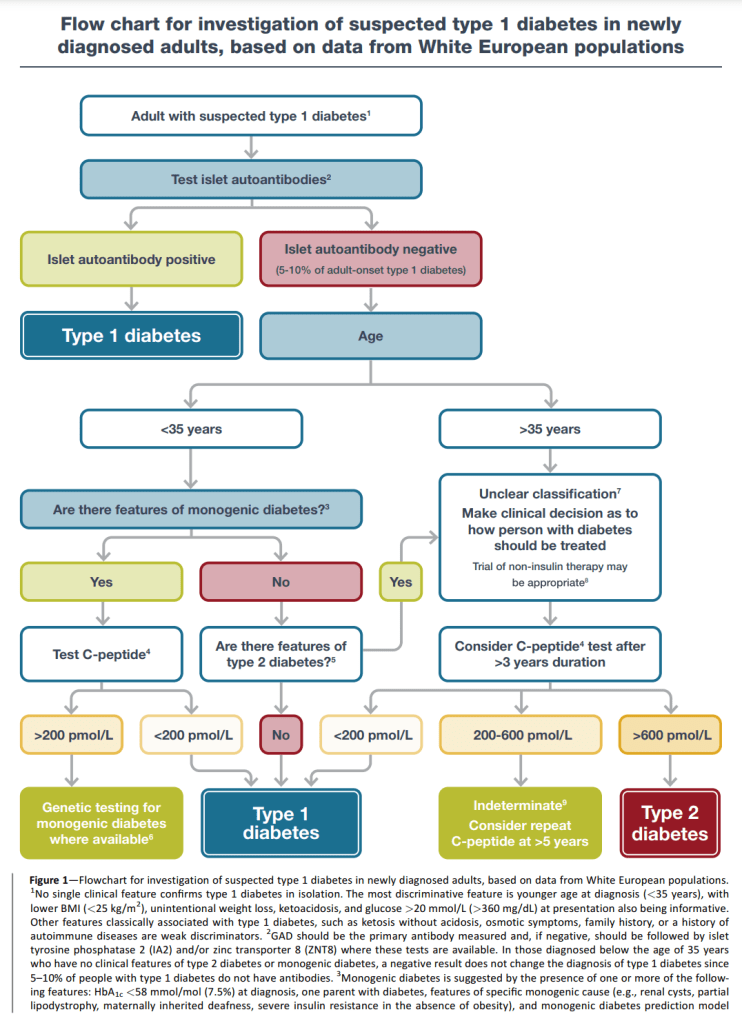

The first statement, like the LADA report, is that no one feature is categorical, not even auto-antibodies (which can be present in other conditions). So, assuming something, such as DKA, has triggered the investigation, testing for auto-antibodies is, like the LADA report, the first place to look. Also, similar to the LADA report, the Type 1 report considers GADA as the first auto-antibody to screen for, followed by the others. If the test is positive, the patient is considered to have Type 1 diabetes.
If the test is negative (as can be the case in 5-10% of people with Type 1), age is the next consideration. For patients over 35 years old, it is not obvious what Type of diabetes they have. The suggestion is assume Type 2 unless there is suspicion of a different Type e.g. Type 3c, but monitor closely for a rapid deterioration in insulin production. After 3 years, test their C-peptide levels (“a random C-peptide measurement (with concurrent glucose) within 5 hours of eating”) and if they are very low (less than 200pmol/L) then they are considered to have Type 1 diabetes. If the C-peptide levels are high (greater than 600pmol/L) the patient is considered to have Type 2 diabetes. If their C-peptide levels are between these two extremes, the recommendation is to re-test in 5 or more years.
For patients who test negative for auto-antibodies and are less than 35 years old, if MODY is suspected, test the C-peptide and if greater than 200pmol/L, perform genetic testing for MODY. If the C-peptide is less than 200pmol/L, the patient is considered to have Type 1 diabetes. Where MODY is not suspected, and there are no indications of “classic” Type 2, the patient is considered to have Type 1 diabetes. While not obvious what the conclusion is for patients with a C-peptide greater than 200pmol/L, one would assume they follow the same path as those over the age of 35.
Reconciling the Two Consensus Reports
The Type 1 flow chart is more complex so we will use this as the foundation and modify it, if required, to align with the LADA flow chart.
In both reports it is directly acknowledged there is no categorical feature to define Type 1 or LADA. For the purposes of diagnosis, this means there must be a reason we are testing for diabetes in the first place. The Type 1 report suggests “unintentional weight loss, ketoacidosis, and glucose >20 mmol/L (>360 mg/dL) at presentation…Other features classically associated with type 1 diabetes, such as ketosis without acidosis, osmotic symptoms, family history, or a history of autoimmune diseases are weak discriminators.”
Assuming some kind of indicator of diabetes is in place, both reports call for screening for the GADA auto-antibody. If this fails, following up with the other indicative auto-antibodies. If any of these are positive then we have a diagnosis of Type 1 and, depending on the C-peptide level, treatment may differ. Given we are dealing with diagnosis and not treatment in this post, let us move to the case of a negative auto-antibody test.
For the LADA consensus report, once all of the auto-antibody tests come back negative, the conclusion is the patient is Type 2. However, the Type 1 consensus report does not give up so easily. As mentioned in the previous section, if the person is under 35, and there is no indication of MODY or Type 2 (high BMI, no DKA and less severe hyperglycaemia), the conclusion is the patient is likely to have Type 1 diabetes.
This last part, where the patient is negative for auto-antibodies, is probably the biggest departure in diagnosis between the two flow charts. Given there is a far higher rate of misdiagnosis of Type 1/LADAs as Type 2 than the other way around, my preference would be to side with the Type 1 report’s process and conclusions. As we will see in my future post on the treatment recommendations of the two reports, the treatment for a person with Type 1 and high C-peptide levels (as can be the case for LADAs), and the treatment for people with Type 2 is quite similar with main difference being the exclusion of sulfonylureas which can accelerate a person with LADA’s progression to insulin dependence.
tl;dr
The two consensus reports are pretty similar with the Type 1 report being the more comprehensive. The main difference is for people who test negative for auto-antibodies. For the LADA consensus report, it is assumed they have Type 2 diabetes whereas the Type 1 consensus report assumes, if there are no indications of MODY or Type 2, the patient likely has Type 1 and should be treated accordingly.
Therefore, whether someone is suspected of having Type 1 diabetes or are part of the LADA sub-group, the Type 1 consensus report’s flow chart is a good guide for accurate diagnosis. The main steps of this flow are:
- Determine there is a reason to suspect some form or diabetes e.g. unintentional weight loss, ketoacidosis, and glucose >20 mmol/L (>360 mg/dL) at presentation
- Screen for GADA auto-antibodies
- If positive, the patient has Type 1 diabetes
- If negative and under 35
- Consider the possibility of MODY and, for a sufficiently high C-peptide level, test if suspected. If negative for MODY (presumably) treat them as if they were negative and over 35 (see below)
- Consider the possibility of Type 2. If the presentation is consistent with Type 2 (high BMI, no DKA and less severe hyperglycaemia) then diagnose them as if they were negative and over 35 (see below)
- If the presentation is not consistent with “classic” Type 2 diabetes, assume they are Type 1 and treat accordingly
- If negative and over 35
- Consider the possibility of other Types but, if there are no other indicators, assume Type 2 diabetes but monitor closely for a rapid drop in insulin production. Test C-peptide levels in 3 years (“a random C-peptide measurement (with concurrent glucose) within 5 hours of eating”). If the C-peptide levels are high, the patient is considered to have Type 2 diabetes, otherwise re-test in 5 or more years

2 thoughts on “EASD 2021: Reconciling the International Consensus Reports for LADA and Type 1. Part 1: Diagnosis”