Being part of the dedoc voices (https://dedoc.org/voices); a group of online advocates for people with diabetes who attend diabetes conferences and pass on what they learn to their respective communities gave me the opportunity recently to attend ATTD 2022, one of the largest and most prestigious conferences in the diabetes research calendar.
I had attended virtually last year and this had the unintended consequence of being added to the conference mailing list. While most emails advertised presentation by conference sponsors, about a year after attending, I received a “call for papers for ATTD 2022”. While not an academic in the field, I wondered if the subject matter of one of my blogs would make for appropriate content at the conference. So I submitted my blogs (here and here) on merging the reconciliation reports for Type 1 and LADA. To my shock and delight, it was accepted as a poster for the event.
Once dedoc discovered my submission had been accepted they also offered to fly me to the conference in Barcelona, Spain to promote my poster at the conference as I was the first dedoc voice who had a poster accepted for the event. Not only would I be participating in the conference, but I would also be there in person, rubbing shoulders with the greatest minds in diabetes research. It was very exciting. I set about putting my poster together which was simpler than I thought. I literally used Microsoft Visio to create the flow diagrams of my poster and Microsoft PowerPoint for the poster itself. It could not have been easier. With the generous help of others in the dedoc community with experience at submitting and reviewing academic medical posters, I put together something worthy of the conference.
The idea behind the poster was simple. In 2020, an international expert panel released a consensus report for the diagnosis and treatment of LADA (Latent Autoimmune Diabetes in Adults), also known as Type 1.5. A year later, the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) released a consensus report for the diagnosis and treatment of Type 1 diabetes. Given LADA is often considered a sub-type of Type 1 it is reasonable to expect the two reports to have consensus with each other, but they did not.
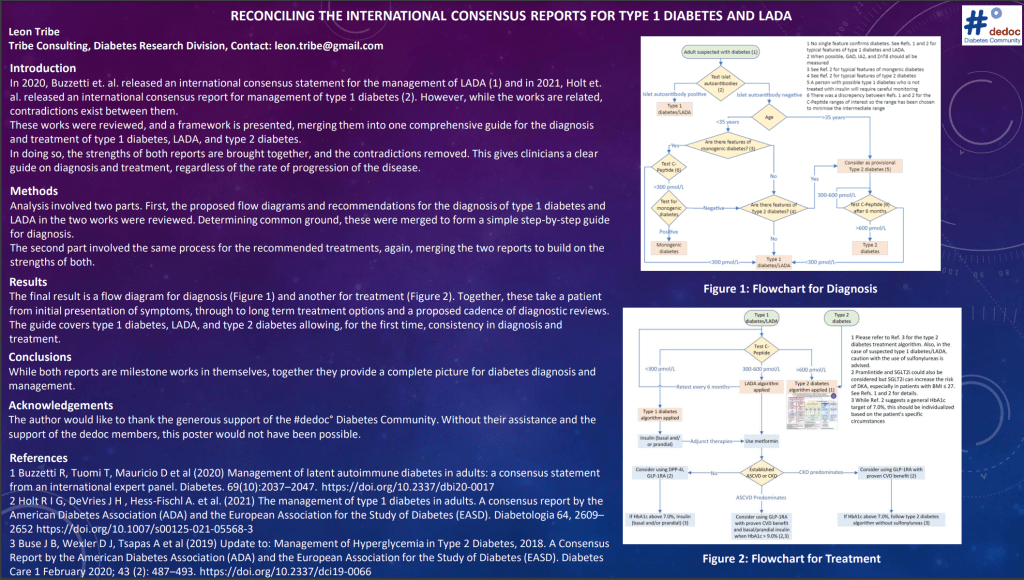
The poster sought to reconcile the two reports and, in doing so provided a flowchart for the diagnosis of diabetes across multiple types of diabetes.
Starting with someone showing classic symptoms of uncontrolled diabetes (thirsty, rapid weight loss, tired, frequent urination) the patient is first testing for auto-antibodies. A positive test immediately confirming Type 1/LADA. If negative, the age of the patient is considered. If they are less than 35 years old, and show signs of monogenic diabetes (MODY) such as a parent with diabetes and a relatively low HbA1c, combined with a medium to high c-peptide level, then genetic testing should be used to confirm or rule out monogenic diabetes. Next, we consider if there are typical Type 2 features such as an increased Body Mass Index. If so, we consider it as ‘provisional’ Type 2 and monitor the c-peptide levels every 6 months. If the c-peptide levels remain above 600pmol/L we consider them Type 2. If the levels drop below 300pmol/L, or there are not features of Type 2 diabetes, we assume it is Type 1/LADA without the presence of auto-antibodies.

For the first time, we have a diagnosis flow diagram for diabetes starting with a patient with symptoms, but an unspecified type, and we move through a series of tests to arrive at a diagnosis of MODY, Type 1/LADA, or Type 2 diabetes. For patients where it is still unclear whether it is Type 1/LADA without auto-antibodies or Type 2 diabetes, we have a clear cadence of checks until the right diagnosis is revealed.
From there, the reconciliation of the consensus reports led to a second flowchart for the treatment of Type 1/LADA and Type 2 diabetes. For Type 2 diabetes, the treatment is as specified in the consensus report for the management of Type 2 (also released in 2020). For Type 1/LADA, the results of the c-peptide 6-monthly checks inform the treatment. If the c-peptide levels are greater than 600pmol/L then the treatment follows the Type 2 protocol, with the recommended exclusion of sulfonylureas. If the c-peptide levels are 300-600pmol/L then the ‘LADA protocol’ is used which recommends the use of metformin with other adjunct therapies, depending on the presence of cardiovascular or chronic kidney disease. These adjunct therapies include DPP-4 inhibitors, GLP-1 receptor agonists and, if the HbA1c is sufficiently high, insulin (basal and/or prandial). If the c-peptide levels are less than 300pmol/L, the ‘Type 1 protocol’ is used which is effectively identical to the LADA protocol but specifies the immediate use of insulin (basal and/or prandial).

In the case of the second flow diagram, we have the basis for a well-defined protocol of treatment for Type 1, LADA, and Type 2 diabetes with treatment modifying as the disease progresses, in the case of LADA diabetes. Moreover, as new diabetes treatments are developed, they can be incorporated into the protocols, based on the evidence for their efficacy.
The importance of the poster is this is the first time we have a set of protocols that any health care provider can follow for the diagnosis and treatment of diabetes, backed by the international consensus of leading authorities. In my opinion these flow charts should be on the wall of the office of every health care professional who treats people with diabetes. While there is still the potential for misdiagnosis and mistreatment, by adopting a common standard, the flowcharts can be constantly improved to maximise the quality of care for people with diabetes.
Overall, I have really enjoyed the experience of putting the poster together and taking it to an international diabetes conference. The next steps are to collaborate with diabetes academics to write a peer reviewed paper on the subject. This will also provide the opportunity to update the recommendations with the latest conclusions from the literature in terms of medications but also in terms of devices such as continuous glucose monitors, pumps and looping technology.
What I have learned from the experience is this poster is proof that the voices of the diabetes community are important and can make a difference, not only in their own communities but on the international stage. We are worthy of participating in all arenas because no one knows diabetes as well as a person living with it. We are all experts of this disease in our own way and our experience and wisdom is important. If you have an idea or potential discovery which can help people with diabetes, do not be held back by doubt but pursue it. I promise you will not regret it.
