In this battle I compare Breezy Packs to breast pads.
Why Breast Pads?
It may seem like a curious choice but there is method to it. In “Frio vs Breezy Packs” I mentioned that Breezy Packs use Phase Change Materials (PCMs) to maintain the internal temperature. For a rundown of the physics on how they work, head over to that post.
While the specific material used in Breezy Packs is a trade secret, one candidate substance is octadecane whose melting point is around 28C (82.5F). While not listed on the box, on eBay the listing for the breast pads had octadecane as one of the main ingredients. For $20 it was worth a shot.
Sure enough, on touching the pad there was a cooling sensation so things were promising.
The Setup
For Breezy Packs, I used their smallest size and put one of my Ozempic pens inside with a digital temperature sensor embedded within it.
For the breast pads, I used a mesh pencil case I had picked up and layered the breast pads inside with another pen with a sensor between them.
In the image you only see the pads on one side but I did put eight on one side and eight on the other for the experiment.
A third sensor was used to track the oven temperature.
With the two containers on a rack on an oven tray (I did not want the tray to be in direct contact with the containers) I placed them in the oven and took the temperature around every five minutes until one of the containers went past 30C (86F).
Prior to entering the oven, the breast pads consistently measured a lower temperature than the Breezy Pack. I assume this was because of the higher area of contact between the pads and the insulin pen. However, things changed when the oven became involved.
The Results
While the breast pads initially showed a lower temperature, this soon changed. Both were pretty stable but, at 17:15, the temperature of the oven was continuing to fall and was heading towards 30C so I increased the dial by a small amount. The different response can be seen with the breast pads increasing temperature much faster than the Breezy Pack and eventually hitting 30C. In fact, over 40 minutes, the breast pad temperature went up by 7C (12F) compared to 2C (3F) for the Breezy Pack.
Conclusions
Breezy Packs wins again although I suspect if we used a similar volume/weight of breast pad PCM the result may have been different. This being said, the amount of breast pads needed to achieve this would be excessively expensive. As with previous experiments, the components were fully funded by myself without commercial sponsorship of any kind.
I had my six-monthly meeting with my Endocrinologist this week and it was clear the atmosphere was a little more formal than usual. Looking over my blood results he asked “Where do you want to start?”. Getting straight to the point I indicated the HbA1c number to which he replied “6.6%”.
This came as quite a shock as, for the five years since diagnosis, I had been 6.1% or less. The number had drifted up slightly in the last few results but this was quite the jump. “Well that’s it”, I concluded, “it is time to get onto the good stuff” which, in this case, meant insulin.
Set Your Goals and Limits Early
Back in November 2019 I had written a blog on what levels a person must maintain to limit damage and the risk of long term complications. My conclusion had been an HbA1c over 6.4% significantly increased the risk of complications and, once I reached this mark, it was time for insulin. That time had come.
I cannot recommend highly enough setting these kinds of personal limits early in your diabetes journey. Talk to your health team, review the literature as I did and create your own lines in the sand. When the time comes, they will serve you well because it is only natural to try and maintain the status quo when, in fact, change is necessary. Let your past self guide your present self so you can both look after your future self.
Grieving the Loss of Familiarity
I am a firm believer people go through grief when faced with significant changes in their life. The move to using insulin while not a big deal in itself, is such a change. While my other medications are to slow the progression of the disease and will no longer be needed in the future, the move to insulin is, in all likelihood, a permanent one.
In reviewing my HbA1c it was tempting to defend the result by considering the large error margin that is inherent in the HbA1c measurement (Denial) but, thanks to my regular reporting for my endo, I knew this result was consistent with the trend of my numbers heading upward and unlikely to be an outlier.
Without my line in the sand of 6.4% it would have also been tempting to give it another, say, six months, resisting my endo’s recommendation for insulin intervention and see where the numbers landed, doing my best to exercise more and eat less sugar in the interim (Pleading, Bargaining, and Desperation) but past Leon had prepared for this day allowing me to move past the second stage, reconciled by evidence over emotion.
There was a little Anger at myself for not doing more e.g. more exercise and less candy but, in reality, the immune system always wins. Five years of insulin independence was a remarkable achievement and it is mentally much healthier to focus on what was achieved than what was not.
There was also a little Depression that the inevitable had arrived along with small feelings of Loss of Self but, again, equipped with the knowledge that this was always going to happen helped me get past this. While there may still be some lingering feelings of this (while I write this it has been three days since I saw the endo), it is time to accept the next stage of my journey.
Acceptance and the Road Ahead
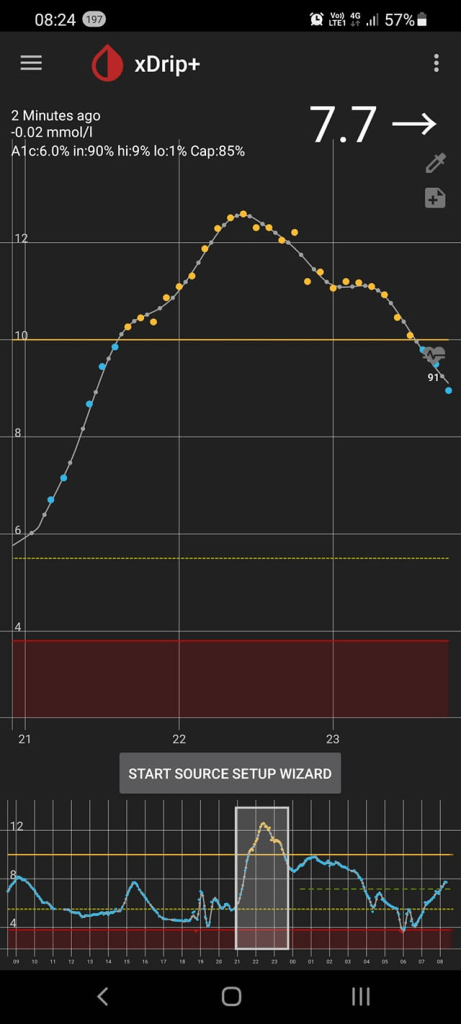
I had put on a sensor in the weeks leading up to the meeting with the endo so we had good information to guide us on where the high sugars were.
It is clear in the trace that from around 9pm at night my numbers go up and slowly drift down until morning. It is also clear that this drift sits around 7 mmol/L (126 mg/dL) and should probably be closer to 5 mmol/L. I remember when I was first diagnosed my blood sugars would sit in the 4s outside of meals but I have not been there for a very long time. This night-time elevation is where we decided to target the levels.
Long Acting Insulin
I spoke about the two main roles of insulin back in 2019. In short, if you are not eating, your levels should be reasonably flat and towards the bottom on the standard range e.g. 4.5-5.5 mmol/L (80-100 mg/dL). If the levels are not behaving like this, it is likely the body is struggling to keep the liver’s glucose release in check. For multiple daily injection, this is the role performed by long acting insulin.
As neither I nor my endo know exactly how much insulin is needed to flatten the overnight curve, we are starting conservatively: 2 units of Levemir taken at around 9pm and monitored once in the middle of the night (checking I am not too low), and once in the morning to see if I am between 4.5 and 5.5 mmol/L.
After one week I will see how it has gone and, if I am not getting down low enough, I will increase the dosage by another 2 units, monitor for another week, rinse and repeat.
There are a few long-acting insulins available but Levemir is useful for my specific purpose because it has peak activity for 12 or so hours which matches the period of time I need it for.
The New Normal
This is now my new normal; injecting once at night and for now, monitoring levels twice per day until I get the dosage right. My new goal is to reduce my HbA1c to a healthier level (sub-6% without hypos would be ideal) and if I can do this without the need for mealtime insulin, even better. Of course, if I continue to have an HbA1c above 6.4%, additional measures will be required. Again, the measures I have set for myself, informed by my own investigations and supported by discussions with my health care team, will guide me and allow me to keep a level head no matter what happens.
I thought I would go through the report I generate for my endo before every visit and the tools I use to create it.
Tool 1: Microsoft Word
All the graphs and tables I generate I put into Word and then save to PDF for emailing.
Tool 2: Nightscout (OOB Reports)
If you are unfamiliar with Nightscout it is, essentially, a web site which shows your CGM’s glucose readings. Very useful for allowing others to review your levels, and used in some looping setups.
For more details on Nightscout, go here. It all might sound technical but the automated scripts make things really easy and no coding knowledge is needed. Also, all the tools it uses are free.
It also comes with a report section which can generate a Glucose Distribution Graph. Generally I select three months for my graphs even if I have not been wearing a CGM for the whole time. This is what the graph looks like.
I am pretty happy with this. Using the conventional TIR range (3.8-10/70-180) I am 93% in range. Given I have not been particularly strict over the last three months, I am good with this. My predicted HbA1c is 6.0% which is creeping up but, given my pancreas is slowly being destroyed by my immune system, this is not overly surprising. Hopefully the blood tests will reflect a similar HbA1c when I get the results back.
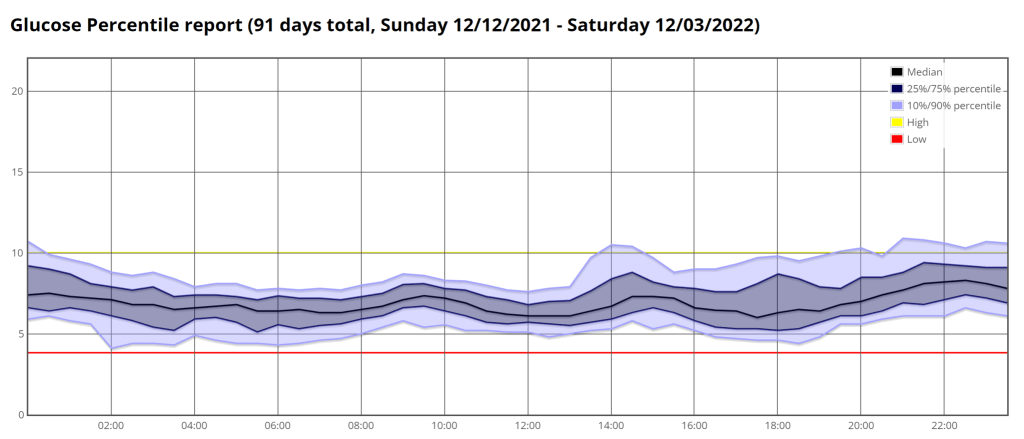
Nightscout also has a Glucose Percentile report showing the spread of values over the day.
Looking at the highs, the areas of interest are night time (around 8pm – 1am) and lunchtime (2pm). In both cases it is likely poor food choices which are to blame. Maybe choosing less carby options at lunchtime will help and maybe I need to be more judicious in my late night snacking.
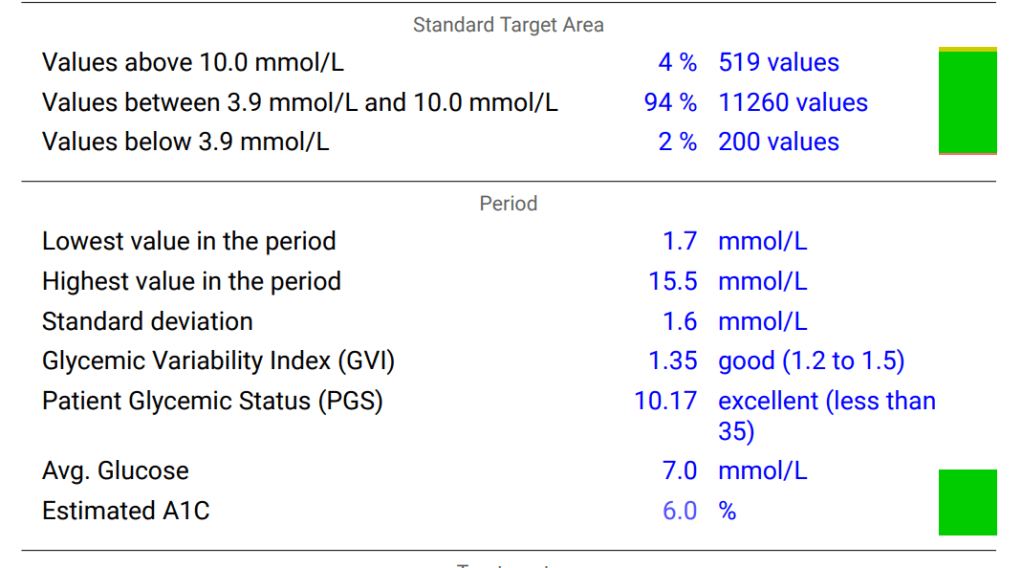
For this tool you will need Nightscout set up. Assuming you have Nightscout in place, you go to the Nightscout Reporter site, give it the web address of your Nightscout site and it does the rest. It also generates a table with similar information to the first graph.
To the casual observer, the “Lowest value in the period” at 1.7mmol/L (30mg/dL) may seem something of concern but this was simply a bad reading from my CGM; it is either a “compression low” (sensor giving a low reading by being squashed) or a worn out sensor giving nonsense readings. Being insulin independent it is impossible for me to go that low. The lowest I have ever been is around 3.5mmol/L (63mg/dL).
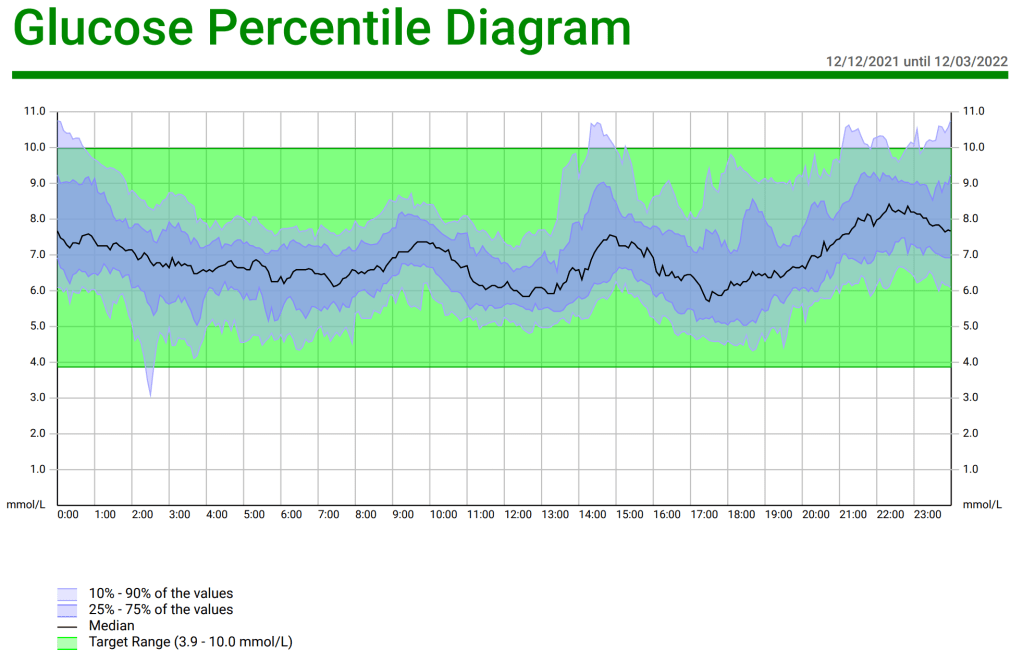
The Nightscout Reporter also has a Glucose Percentile Report but, as it is essentially a repeat of the same report from Nightscout reports, you only need one of them.
The next report I include in my report to my endo is the Comprehensive Glucose Pentagon. It is a spider graph of five parameters us people with diabetes need to keep an eye on and compares it to the typical values for a Muggle (non diabetic person).
For me, the outlier is the CV %, the variability in my glycaemic values. Again this suggests maybe less sweet treats and more lower GI options.
Finally, the Nightscout Reporter gives us a distribution graph of glucose values.
This also gives us a good indication of where our numbers sit.
Medications and Questions
Finally in my report to the endo I include a list of my medications and supplements, and any questions I have. Given my questions often involve new medications or protocols it seems fair to give my endo some notice before meeting them so they can do some research beforehand.
Longitudinal Analysis
The other benefit of generating these reports is I can review the results over time. For example, here are the results of my glucose distribution for 13/08/20-13/11/20, 17/06/21-14/09/21, and 12/12/21-12/03/22
13/08/20-13/11/20
17/06/21-14/09/21
12/12/21-12/03/22
If we look at the “Values above 10.0mmol/L” (180mg/dL) we see this is slowly increasing but still substantially less than the 25-30% guideline.
While the standard deviation is the same, the GVI is increasing suggesting less blood glucose control, but still in the “good” range.
Average glucose is also rising over time.
All of this is consistent with a LADA’s slowly deteriorating pancreas. The question will be when do I start looking at additional interventions, such as insulin? As per my analysis on when damage starts to accumulate, I am happy to let things progress until my HbA1c gets closer to 6.5% but this is also a good subject to discuss with my endocrinologist at my appointment.
This week was my fifth diaversary. It is a word you will not find in the dictionary and is used exclusively in the diabetes community. In short, it is five years since I was diagnosed with Type 1 diabetes.
It may seem a strange thing to celebrate, the acquisition of a chronic, damaging, sometimes fatal disease but it is important, at least to me.
To celebrate I went all out with Italian:
Half of a 14″ meat-lovers pizza
4-inch square of lasagne
half a garlic bread roll
single serve of tiramisu
A nightmare to manage for most Type 1s. Being a honeymooning LADA, albeit an insulin-independent one, helped although I still spiked, peaking at around 12.2mmol/L (220mg/dl) and then headed down.
So why subject my body to such a stress? Because sometimes it is the healthiest thing you can you do for yourself.
My Usual Eating Routine
I characterise my diet at “lowish carbohydrate”. Where there is an obvious, practical low/no carbohydrate alternative to a food, I will eat it. I do not drink sugary drinks, opting for the ‘diet’ alternatives. I am very comfortable with sugar substitutes such as phenylalanine and sucralose. As a general rule I try to make sure anything solid I eat has 10% net carb or less and, for liquids, zero carbs. That is it.
The result, when I stick to this, are blood glucose traces like this.
The thing is, even with these relatively light rules, it still requires commitment and effort to maintain. If I am eating out, I need to scan the menu for the friendliest options. I need to make sure, if I order a soft drink, that the diet version has been served and not its sugar-filled cousin and so on.
Other Common Eating Regimens
Other common eating regimens for people with diabetes are even stricter. If we consider Bernstein’s approach we are eating:
30g of net carb or less per day
Roughly the same amount of carb every day for breakfast, lunch, and dinner e.g. 6g, 12g, 12g
Eating at roughly the same time every day
That is a lot to keep on top of and while I am sure the ‘Gritters’ will say it is not a big deal and worth it because “we deserve normal blood sugar levels” there is no doubt it does require effort and will impact social interactions with those not complying with this routine.
The strictest of all is probably the zero-carb carnivore diet. This pretty much speaks for itself; if it was not once part of an animal (or is a drink with practically no calories) it is off the list.
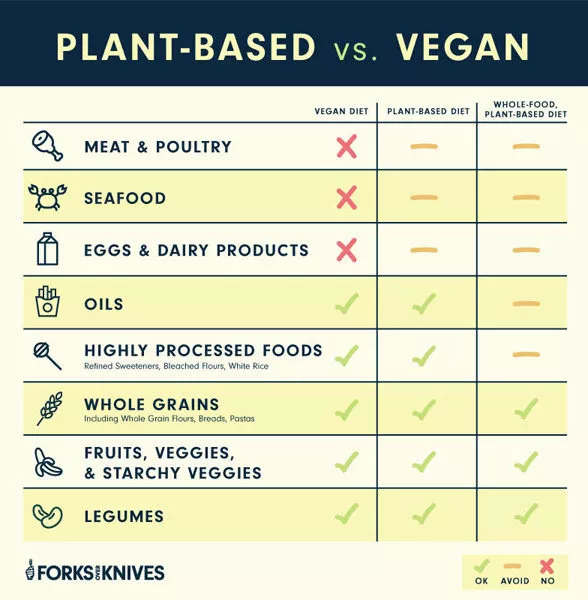
At the other end of the spectrum we have the Forks Over Knives advocates, where eating involves a “plant-based diet”. In short a “small v” vegan diet where no foods are off-limits but some (those from animals) are to be avoided.
This one is relatively friendly and, for those looking to reduce insulin resistance the benefits of avoiding animal fats may outweigh the additional carb intake.
Whatever system that is followed, assuming a person with diabetes is adopting some kind of food management, rules mean conscious effort.
The Risk To Mental Health
Orthorexia nervosa is defined as “an unspecified feeding or eating disorder characterized by an exaggerated, unhealthy obsession with healthy eating”. “The affected individual might be driven by dietary asceticism, cherry-picked evidence, or even by evidence-based recommendations, leading to a restrictive dietary pattern in pursuit of improved health”. Overly strict diets which individuals religiously follow, and myths about the food we eat feed, reinforce this kind of unhealthy thinking.
Another aspect is willpower (also known as volition) is a finite resource. A person can only perform conscious actions for so long before they need to take a break. A person with diabetes is ‘on’ 24-7 (except possibly the closed loopers but they are still the exception rather than the rule). They know that maintaining their blood sugar is necessary to stay alive and stay healthy. So what happens when they run out of willpower to manage their disease? Diabetes Burnout. They simply stop managing the disease because they need to take a break.
Obviously there is a lot more to managing diabetes than food intake but it certainly contributes and can be overly burdensome when it becomes all-consuming.
Food Myths Which Contribute To Orthorexia And Diabetes Burnout
There are a few myths when it comes to blood sugars and food which focus on 140mg/dl (7.8mmol/L)
“Damage Starts Happening When Your Blood Sugar Goes Over 140mg/dl”
I tackled this in a previous blog. In short, there is no evidence that damage begins over 140mg/dl. There is literally no study which has examined people with blood sugars at 141mg/dl and observed cellular damage occurring. It is a myth used to sell books but has no basis in scientific fact. It is true that having a sustained high blood sugar will do damage in the long term but this is better measured through metrics such as the HbA1c or Time in Range (TIR).
“Muggles (Non-Diabetic Folk) Never Go Above 140mg/dl”
This is simply not true. A recent article gave a great summary of some of the research that has been done in this area. Here are quotes from the studies examined:
Muggle Study #1: “On average, their daily glucose levels stayed between 70–140 mg/dl for 93% of the day, with very small portions of the day spent above 140 mg/dl or below 70 mg/dl”
Muggle Study #2: “Levels were lower than 70 mg/dl for 1.7% of the time and greater than 140 mg/dl, only 0.4% of the time.”
Muggle Study #3: “Participants spent 93% of time between glucose values of 70-140 mg/dl, with 3% of the time below 70 mg/dL on average and 4% of the time above 140 mg/dl on average”
Muggle Study #4: “2.1% of glucose sensor values were >140 mg/dl”
Muggle Study #5: “Glucose was above 140 mg/dL for only 0.8% of the day”
Muggle Study #6: “Participants spent 1.6% of the time above 140 mg/dl”
Literally every study showed that while going above 140mg/dl was the exception, even Muggles do it for short periods of time every day.
In other words, not only are these myths untrue, anyone believing them is putting themselves under unnecessary mental stress for effectively no discernible gain.
Diaversary As A Mental Steam-Release Valve
This is why I celebrate my diaversary. My diaversary is a day when I give myself permission to not to be as concerned with my blood sugars, secure in the knowledge that one day of spiking is going to do little but give me a mental break and help me recharge for the other 364 days. I genuinely believe the one day of poor bloods is a small price for sustained mental wellbeing. While maintaining healthy blood glucose levels is important, so is managing my mental health. My diaversary is a key element in my approach.