I thought I would go through the report I generate for my endo before every visit and the tools I use to create it.
Tool 1: Microsoft Word
All the graphs and tables I generate I put into Word and then save to PDF for emailing.
Tool 2: Nightscout (OOB Reports)
If you are unfamiliar with Nightscout it is, essentially, a web site which shows your CGM’s glucose readings. Very useful for allowing others to review your levels, and used in some looping setups.
For more details on Nightscout, go here. It all might sound technical but the automated scripts make things really easy and no coding knowledge is needed. Also, all the tools it uses are free.
It also comes with a report section which can generate a Glucose Distribution Graph. Generally I select three months for my graphs even if I have not been wearing a CGM for the whole time. This is what the graph looks like.

I am pretty happy with this. Using the conventional TIR range (3.8-10/70-180) I am 93% in range. Given I have not been particularly strict over the last three months, I am good with this. My predicted HbA1c is 6.0% which is creeping up but, given my pancreas is slowly being destroyed by my immune system, this is not overly surprising. Hopefully the blood tests will reflect a similar HbA1c when I get the results back.
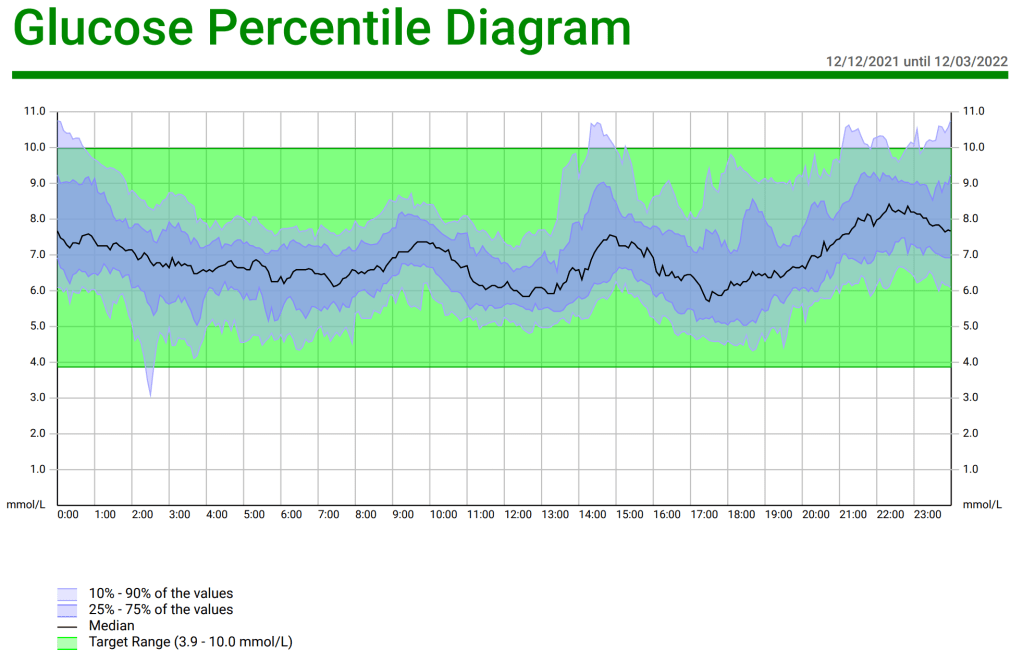
Nightscout also has a Glucose Percentile report showing the spread of values over the day.

Looking at the highs, the areas of interest are night time (around 8pm – 1am) and lunchtime (2pm). In both cases it is likely poor food choices which are to blame. Maybe choosing less carby options at lunchtime will help and maybe I need to be more judicious in my late night snacking.
Tool 3: Nightscout Reporter (https://nightscout-reporter.zreptil.de/)
For this tool you will need Nightscout set up. Assuming you have Nightscout in place, you go to the Nightscout Reporter site, give it the web address of your Nightscout site and it does the rest. It also generates a table with similar information to the first graph.
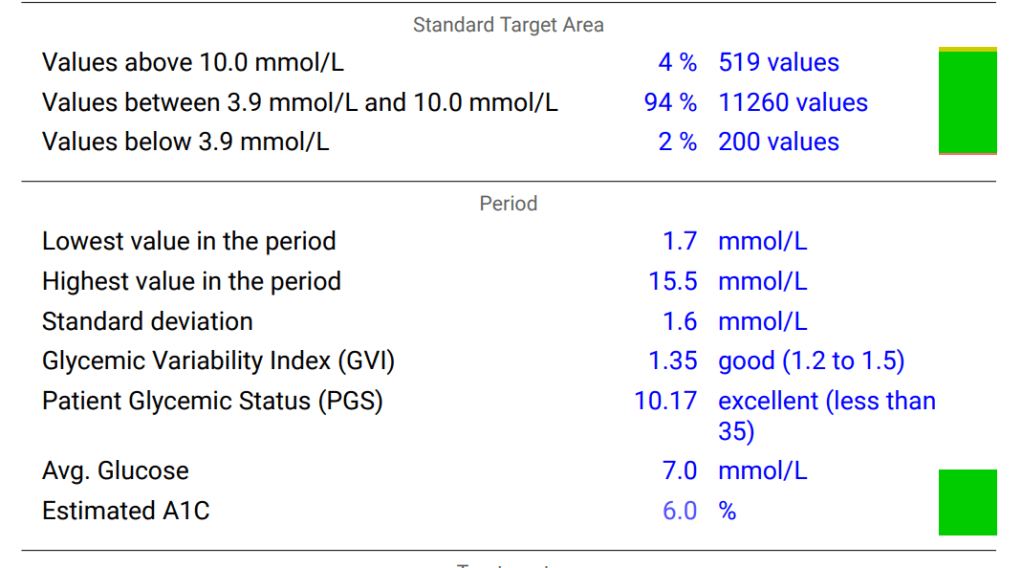
To the casual observer, the “Lowest value in the period” at 1.7mmol/L (30mg/dL) may seem something of concern but this was simply a bad reading from my CGM; it is either a “compression low” (sensor giving a low reading by being squashed) or a worn out sensor giving nonsense readings. Being insulin independent it is impossible for me to go that low. The lowest I have ever been is around 3.5mmol/L (63mg/dL).
The Nightscout Reporter also has a Glucose Percentile Report but, as it is essentially a repeat of the same report from Nightscout reports, you only need one of them.
The next report I include in my report to my endo is the Comprehensive Glucose Pentagon. It is a spider graph of five parameters us people with diabetes need to keep an eye on and compares it to the typical values for a Muggle (non diabetic person).

For me, the outlier is the CV %, the variability in my glycaemic values. Again this suggests maybe less sweet treats and more lower GI options.
Finally, the Nightscout Reporter gives us a distribution graph of glucose values.

This also gives us a good indication of where our numbers sit.
Medications and Questions
Finally in my report to the endo I include a list of my medications and supplements, and any questions I have. Given my questions often involve new medications or protocols it seems fair to give my endo some notice before meeting them so they can do some research beforehand.

Longitudinal Analysis
The other benefit of generating these reports is I can review the results over time. For example, here are the results of my glucose distribution for 13/08/20-13/11/20, 17/06/21-14/09/21, and 12/12/21-12/03/22
13/08/20-13/11/20

17/06/21-14/09/21

12/12/21-12/03/22

If we look at the “Values above 10.0mmol/L” (180mg/dL) we see this is slowly increasing but still substantially less than the 25-30% guideline.
While the standard deviation is the same, the GVI is increasing suggesting less blood glucose control, but still in the “good” range.
Average glucose is also rising over time.
All of this is consistent with a LADA’s slowly deteriorating pancreas. The question will be when do I start looking at additional interventions, such as insulin? As per my analysis on when damage starts to accumulate, I am happy to let things progress until my HbA1c gets closer to 6.5% but this is also a good subject to discuss with my endocrinologist at my appointment.

I love especially the reports from Nightscout Reporter as they display everything I need. As you can personalise them and even save your settings for the personalised graphs you need it makes it easy to generate them quickly! 😉
LikeLike
Hi Leon. I am on a similar LADA journey. I worked very hard (including using exercise and alcohol extensively) for years to manage my glucose levels “like a type 2.”
I did not want to “resort” to insulin. And I put it off longer than I probably should have in hindsight.
When I finally decided to give Afrezza inhalable insulin a try (available in the USA) it really changed my perspective on how different life would be using insulin. Before considering Afrezza, I was really concerned about dosing, needles, pumps’n’tubes, and all the more troublesome aspects of being insulin dependent, but with Afrezza, virtually all of these issues faded away. And, even better, I am able to control my glucose levels far more accurately than I could using my “type 2” regimine. And with virtually no downside, pain, or interruptions to my life compared to my life before insulin.
In fact, I don’t even consider it insulin from a mental model perspective, because insulin is lodged in my – and everyone’s – conscious as an injected substance that requires a lot of care and planning to get right with every dose (or an attached device that does it for you). This is just not the case with Afrezza. Due to the nature of delivery, I feel it’s more akin to being asthmatic than diabetic from a mental model perspective.
Just something to consider as you look at LADA’s slow-but-steady reduction in insulin production…
Cheers.
LikeLike
I’m a big fan of Afrezza but, as you allude to, it is not available here in Australia. It is hard to know when is the right time to bring insulin into the mix and a simple, fast-acting inhalable insulin with, anecdotally, less risk of hypo/rollercoasting is a compelling prospect.
Given this is not an option, I set measures early on where, when I reach those targets, I’d move to insulin. For me, it is an HbA1c of 6.3% or more, based on the review in this article (https://practicaldiabetic.com/2019/11/06/above-what-level-does-your-hba1c-fasting-glucose-and-glucose-spikes-do-damage/) and this was the primary driver for reviewing all those papers.
If there was evidence that every spike above 140mg/dL did damage I would be on bolus insulin for every meal. Fortunately there is not evidence of this. There is no doubt though, the higher the HbA1c, the higher the risk of long term complications. For me, 6.3% is the line in the sand which gives me enough buffer to manage the fluctuations while I get used to my new medication.
Whether that will be bolus insulin or basal will be informed by my CGM traces; if my base glucose line is too high with minimal prandial fluctuations, basal will be used and vice versa. What I do know is, once I am there I intend to get onto looping as soon as possible and get my HbA1c as low as possible without exposure to severe hypos. 6.3% may be my turning point but it is certainly not the final destination. I see it more as an unacceptable upper limit.
While 6.3% is good for me, and we see this on the forums we both are on, for others this is unacceptably high. That is their journey and I wish them all success in it. ADA set their upper limit HbA1c at 7.0% but make it clear the target needs to be individualized. I try to balance the burden of management with health risk management and management cost in alignment with my life and other commitments. Obviously everyone will have different factors in play in that regard.
LikeLiked by 1 person
Research is a great place to start, but just like any other physiological dynamic, each of us responds to environmental factors uniquely. Some people are more sensitive to variations and extreme than others. It’s possible that you and I happen to be less sensitive to extremes of glucose toxicity than others. Or we might be more sensitive. My dad is almost 85 and has been insulin-dependent since 28. You know that at that age, he wasn’t managed well most of his life. He does have the classic complications, but the fact that he’s alive speaks much to his ability to endure these glucose toxicity extremes he’s been exposed to.
Unfortunately, none of us will know until it’s virtually too late how sensitive or immune each of us are to glucose toxicity (or high cholesterol or blood pressure, or any number of other physiological dynamics), so I personally prefer to play things conservatively. My endo happens to believe that under 6% A1c is the safe zone. I prefer to stay under 5.7% A1c. As you say, to each his/her own. We all own our own journey.
It’s weird and a shame that Afrezza isn’t available outside the U.S. It’s a stupendous innovation that every diabetic (type 1 and type 2) should have access to. Needles are barbaric. Inhaling reduces the invasiveness of this condition by an order of magnitude. I’d lobby for it if I were you.
LikeLike