I had the privilege of being a Dedoc Voice in Berlin at ATTD 2023 this year. While there were many fascinating discussions (many of which I Tweeted about at PracticalDeeb) there was one in particular that really stood out and that was a frank and open discussion on the clinical relevance of Time in Range and whether it needs revising.
For those who want to cut to the chase, there is a tl;dr at the end.
What is Time In Range (TIR)?
Before launching into the presentations at ATTD, it is probably best to explain the term Time In Range. Thankfully, I have already written a piece explaining it, using a presentation from EASD 2020 by Professor Pratik Choudhary (who was my t-shirt hall of fame recipient for the conference).

In short, the default standard is the range 70-180 mg/dL (3.9-10 mmol/L) and the traditional target was to reside within this range for more than 70% of the time, as measured by a Continuous Glucose Monitor (CGM).
This presentation at ATTD 2023 put the target under the microscope to see if it needed revising.
Time in Tight Range: The New Standard?

Professor Thomas Danne introduced a concept of a Time in Tight Range (TITR) which reduces the range to 70-140 mg/dL (3.9-7.8 mmol/L). Why a new range? Because Professor Danne literally said “I don’t want to lie any longer”.

The suggestion was, to live a normal, healthy life, 70% TIR was not enough but to give truth to what needs to be achieved would discourage when encouragement was needed so a “soft target” was given instead. This admission will vindicate many online pundits who rail against TIR as insufficient to avoid complications. In essence, this has now been confirmed.
An advantage of considering TITR is spikes, which may remain within TIR but not TITR, can be identified and worked on, assuming managing levels within TIR has been achieved.
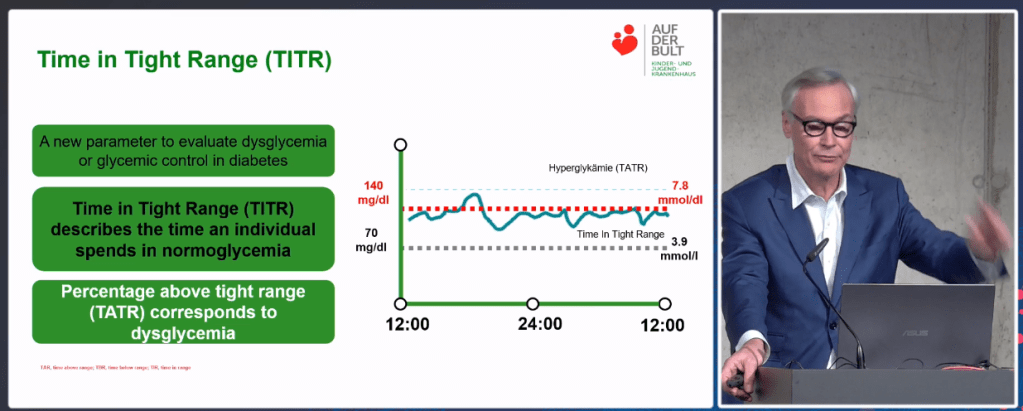
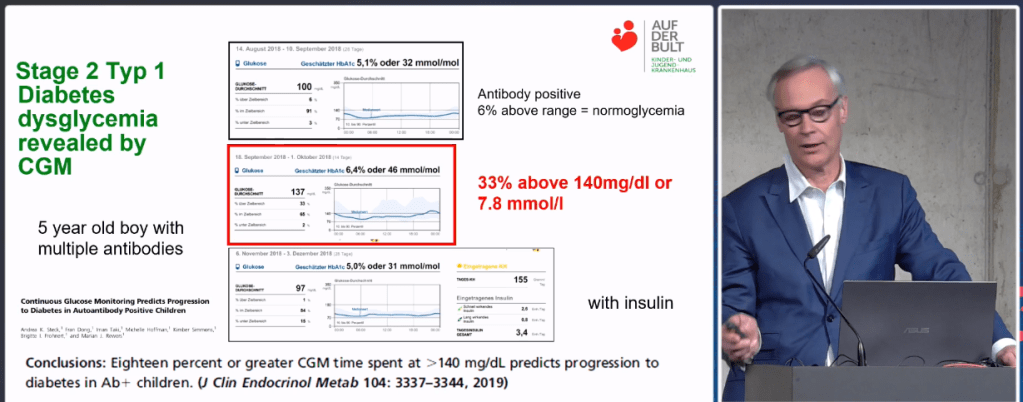
It is interesting to note that Professor Danne considered 70-140 as “normoglycemia” i.e. normal blood sugars and above 140 as “dysglycemia” (not normal blood sugars) and therefore concluded TITR can also be used as a range for early detection i.e. Stage 2 Type 1 Diabetes (when blood glucose levels are not normal but insulin is not yet being used). Professor Danne also cited a paper that concluded that time above the tight range predicted the progression to Stage 3 Type 1 Diabetes i.e. when insulin is required.
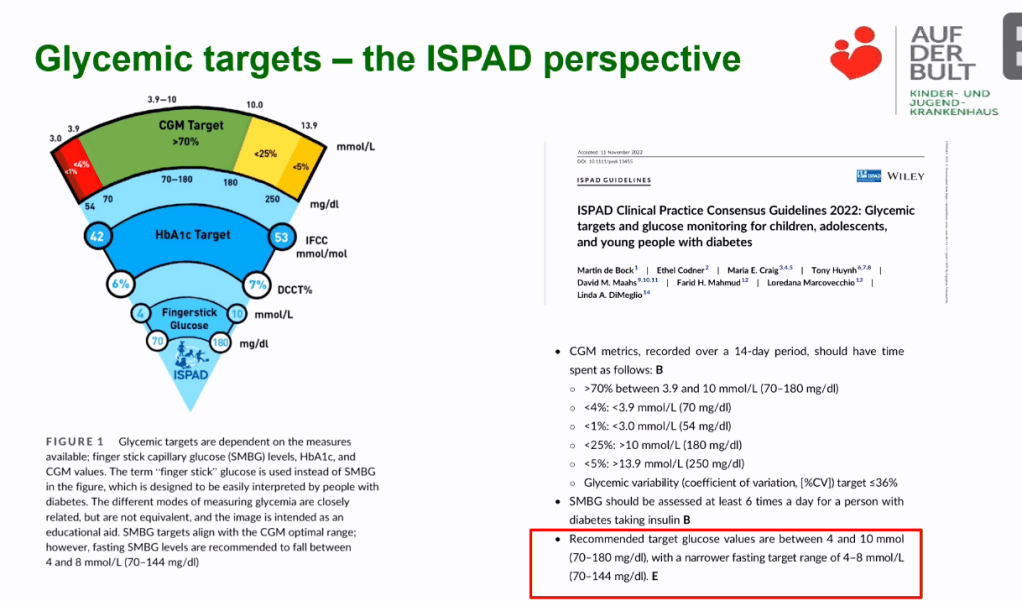
Professor Danne went further and stated he felt the latest ISPAD Time in Range guidelines do not go far enough, claiming the life expectancy of a child with type 1 diabetes will not be the same as a child without type 1 diabetes using these targets.
His preferred goal? An ambulatory glucose profile characterised as “Flat, Narrow, and In Range” (FNIR).

The Gritters can raise a glass of alcohol-free, non-fizzy coconut milk and celebrate that academia is beginning to align to their strict goals. So did Professor Danne go on to talk about all people with type 1 diabetes adopting an ultra-low carbohydrate diet, and eating a strict three meals a day? Well, no.
As alluded to earlier, his goal is to provide guidance to people with diabetes and their carers which is considered achievable and sustainable, even if this means historically softening the targets. Also, Professor Danne made it clear a qualitative daily target was insufficient but a SMART (Specific, Measurable, Achievable, Relevant, and Time-Bound) goal was also needed i.e. quantitative as well as qualitative. His solution? Automated Insulin Delivery i.e. Looping.

His evidence that AID leads to improved results? A comparison across countries of HbA1c pursued through various means compared to Time in Range pursued through AID. Even in the best performing country (Sweden) people with type 1 diabetes struggled to get an HbA1c below 7% (50 on the scale). However, all countries consistently achieved a TIR above 70% which is broadly equivalent to an HbA1c of 7% using AID.

But are we not considering TITR, not TIR? Alas reporting on TITR is still quite limited but Professor Danne is hopeful. On top of using AID, he also mentioned the results being achieved with SGLT2i drugs (which basically redirect glucose in the blood to the bladder, keeping blood glucose levels low).

The jury is still out on the use of SGLT2i’s in people with type 1 diabetes because of the increased risk of eDKA but Professor Danne is hopeful, the rise of continuous ketone sensors will address this. For someone like me who still has residual pancreatic function, the use of an SGLT2i is more compelling because the residual insulin means any form of DKA is extremely unlikely.
More evidence of the superiority of AID over other methods came from a Cambridge study which showed improved sustainable performance over two years.

Doctor Peter Adolfsson continued the story by presenting on the specifics of what those SMART goals should be.

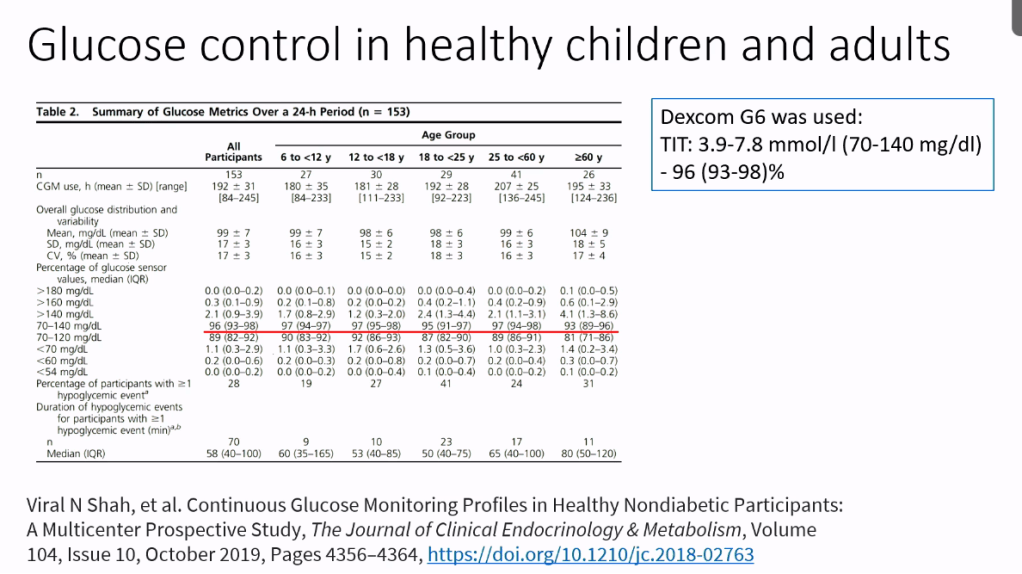
First he talked at what normal blood sugars in children look like where the TITR is close to 90%
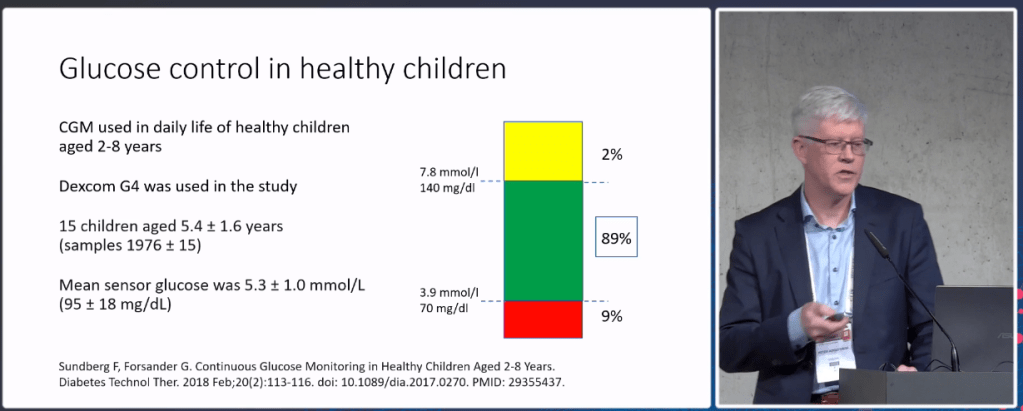
A more recent study with more accurate CGMs puts the number at 96% TITR
Doctor Adolfsson then moved the discussion to what target do we need to achieve, not to match people without diabetes, but to reduce the risk of complications to match the non-diabetic population and suggested an HbA1c of 6.5% was sufficient for this which corresponded to a TITR of 50%. This comes close to the conclusions I came to a while ago that an HbA1c under 7.0% is good but, if it can be achieved without severe hypo risk, an HbA1c of 6.4% is better.

tl;dr
Professor Danne acknowledged that, historically, advice to people with type 1 diabetes had been targets which still exposed them to long term complications because it was simply too hard and arduous for the client to achieve tighter targets i.e. the goal was harm minimisation rather than elimination. However, the advent of Automated Insulin Delivery (AID) / Looping has meant it is much easier to achieve superior results with minimal additional effort.
This has led to the consideration of the Tight Time in Range (TITR) which puts the goal for glucose levels to be between 70-140 mg/dL (3.9-7.8 mmol/L). This new range has the potential to be diagnostic of the stages of type 1 diabetes as well as provide improved guidance for glucose control.
In terms of the percentage of time to aim for in the new range, for truly normal blood sugars, the target is 96% of the time. However, there is no evidence that can be achieved through AID. The compromise target is to aim for a percentage which reduces the risk of complication to that similar to the non-diabetic population. Research suggests this lowers the target percentage to 50% TITR which corresponds to an HbA1c of 6.5%.
In other words, rather than pursue the goal of “normal blood sugars”, the goal is “free of long term complications”. What I personally like about this approach is TITR can be measured, at home, by anyone with a CGM (unlike HbA1c). Also, the individual can choose how strict they want to be in pursuing “normalcy” i.e. sit at 50% TITR and minimise the risk of complications or go harder to achieve the blood glucose levels of a person without diabetes. This latitude in the percentage allows flexibility in terms of the individual’s personal circumstances which, in turn, minimises the risk of burnout.

Thank you Leon for this great article and summary of this session. I am personally a bit sceptical towards this TITR…it is only achievable by using at least CGMs or better AID systems… these are not available in most parts of the world. Using this technology you will be able for sure. As I have a lot of contacts to the looping community I often see very ambitious people. They really try very hard to achieve best possible results…trying to achieve 100% TiR. And this at the cost of loosing the freedom the loop system was supposed to give them.
So my fear is a bit, that using this TITR will push these eager people even more and lead to augmentation of pressure which might cause even more distress instead of reducing it.
LikeLike
I agree, without access to the technology we are where the presentation began, picking softer targets to strike the balance between harm minimisation and achievability.
Like you I believe perfection is the enemy of good. We need to do our best in our endeavours but to use the singular measure of TIR, rather than a multi-faceted measure involving one’s whole life, means succeeding in one place but almost certainly failing elsewhere. Like with many things, moderation and compromise are key.
For me, a target of 50% TITR, instead of 70% TIR is not a huge shift and I think many people will already be achieving this target and, hopefully this will give them comfort when there are so many sources online focusing on what they are failing to do, rather than on what they are achieving.
Ultimately each person needs to find the targets which make sense for them. For some it will be complete risk elimination, for others it will be wearing a little bit of risk but ensuring they get regular check-ups to catch complications early when they can likely be treated. Depending on the access to technology, and the many, many factors in our life, there will never be one size which fits everyone.
LikeLike