A little over a month ago I wrote how I was starting long-acting insulin at night and beginning the journey of finding the right level.
The good news is I have started to achieve gluco-normal levels in the morning and I am so excited I thought I would write about the path to get there.
The Background
A couple of years ago I did a literature review to work out at what blood glucose levels damage is being done to my body. The conclusions out of that were:
- There is NO evidence that occasionally going over 140mg/dL (7.8 mmol/L) does damage. None, zero, zilch. So stop beating yourself up over a “bad day”. The damage to your mental health is not worth it. Win the war and do not focus on the odd battle that goes astray.
- Keeping your HbA1c below 7.0% is good and, if you are at low risk of hypo, below 6.4% is better. Arguably, the lower you can go without exposure to serious hypos is a good thing
- A fasting blood glucose below 120mg/dL (6.7mmol/L) is a good thing although the best predictor is HbA1c
My last blood results had an HbA1c of 6.6% and a fasting glucose of 7.2mmol/L so things had to change. This is where Levemir came in.
The Choice Of Treatment
I could shortcut to simply using a pump and continuous glucose monitor (CGM) which, in an ideal world, talk to each other to manage my blood glucose levels but, as I still do not require mealtime insulin, and that is a lot of equipment to manage (and pay for given CGMs are not yet subsidized for most people with Type 1 diabetes in Australia), I opted for a simpler solution of taking a long-acting insulin at night.
The insulin suggested by my endo was Levemir. While there are 24-hour insulins available (and weekly ones coming soon), the problem was overnight highs (confirmed by wearing a CGM a couple of weeks up to my endo appointment). We can see this in the excursions above 10 in the below plot which happen, almost exclusively, post dinner and continue until after midnight.

Levemir, with a roughly 12 hour action was a good choice.

Working Out The Dosage
The fact is there is no way to work out the right dosage without experimenting. Too little and blood sugars remain high, doing damage over time. Too much and you hypo which is dangerous and damaging. To quote a meme.

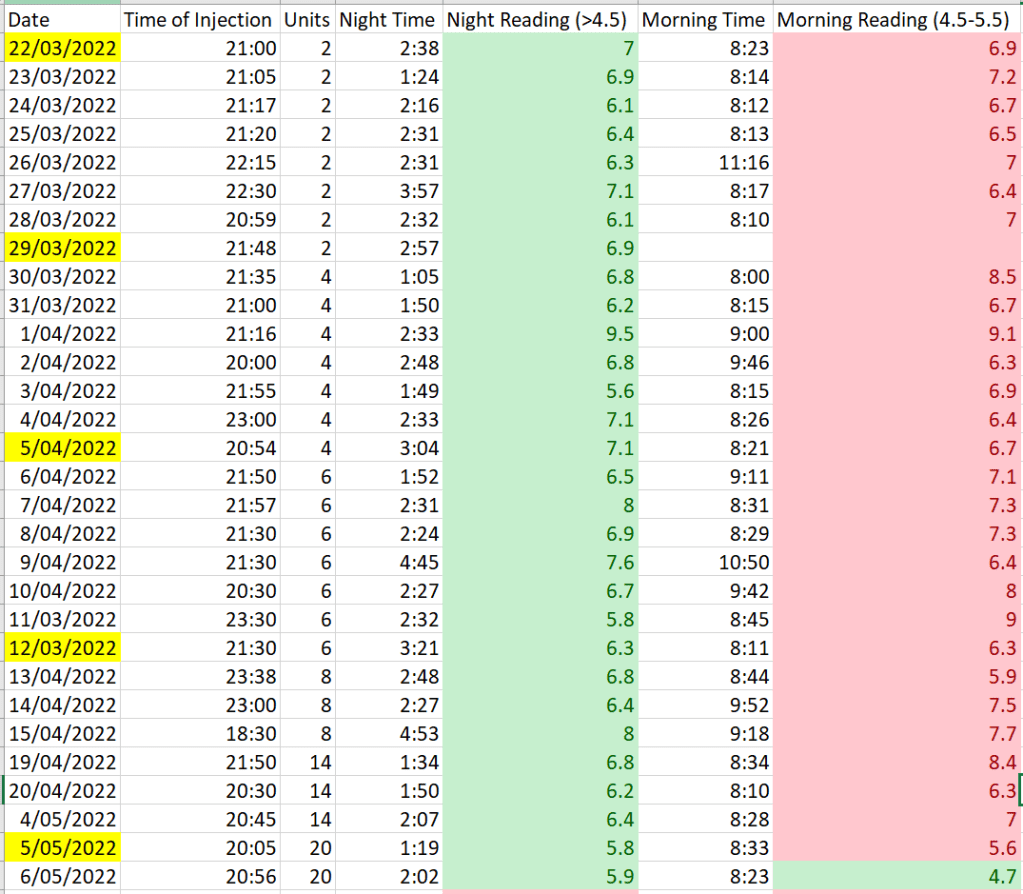
At my endo’s recommendation I started at 2 units and took measurements in the middle of the night and in the morning with a view of keeping the measurement in the middle of the night above 4.5mmol/L (80ish mg/dL) and between 4.5-5.5mmol/L (80-100mg/dL) in the morning. Each week I saw if I was in the goal range and, if not, incremented by 2 additional units.
This went on for a month but it was clear even 8 units was not doing much at all for my blood glucose levels. Clearly insulin resistance (which I knew I had) was working against me. My endo suggested jumping to 14 units and when this did not work, I went to 20 units.
Success!
This morning, for the first time in a long time, my morning blood glucose was in the set range.
Next Steps
Next is to fine tune the units to keep the average around 5.0mmol/L (90mg/dL) and minimise the variation. To measure this I will be looking at the 7-day average for the night and morning readings and the standard deviation. Both of these are readily calculable in Excel. My hope is adjusting the dosage and being reasonably strict on when I inject will keep these measures in check.
Conclusions/Things I Have Learned
- Set your targets/goals early in your diagnosis: It is very easy to put off making a move to insulin, convincing yourself you will move more and eat less and it will all be better in 3-6 months time. I believe a better approach is have your past self set the goals for you when it is less likely emotion will influence the decision. It is also much harder arguing with your past self than it is with an endo who you can dismiss as not knowing your ‘lived experience’.
- Tread carefully but purposefully: While it took a bit over a month to get near the right dosage, the approach was safe in the short term and set me up well for the long term
- Continue to monitor, measure and improve: Getting my levels right now, and monitoring for change will set me up well for when I move to a pump and ensure I remain as healthy as possible. Injecting once a day and measuring twice a day seems like a small price to pay to minimise the risk of long term complications and short term hypos.

I’m astonished that CGMs are not subsidized by your government insurance plan. That said, Freestyle Libre’s are not all that expensive with manufacturers discounts and might be better for ongoing management well prior to needing a pump.
LikeLike