With more looping systems coming to the market from the major manufacturers, there is more research being done into their efficacy, which is great. The focus of a few presentations at EASD 2020 was the benefit of looping systems for Type 1 children and adolescents. What was very interesting was they all came to similar conclusions. This blog will give a summary of those conclusions. Tl;dr available at the bottom for those who do not want to read the details of the individual studies.
Presentation 1: Glycemic Control Improves Over 4 Month Use of Closed Loop Insulin Delivery in School-Age Children with Type 1 Diabetes
Presented by Dr. Marc Breton.
For this study the t:slim X2 with Control-IQ was used over 16 weeks. 100 children participated between the ages of 6-13 and none had used looping before.
The results were all positive. For Time in Range, there was an improvement over the control group. The control group was one quarter of the participants using a pump with no looping.
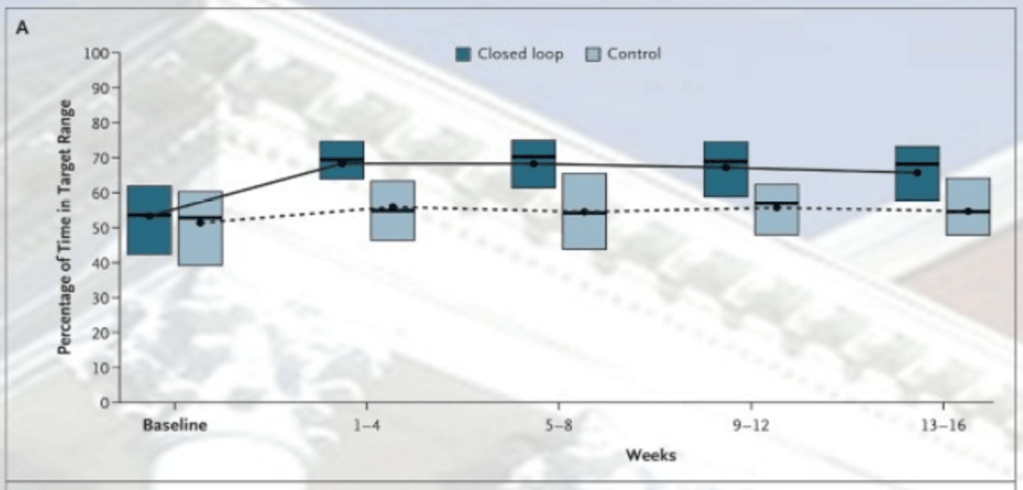
From other presentations at EASD 2020, there is evidence to back up the assertion that a Time in Range (70-180mg/dL aka 3.9-10 mmol/L) of 70% or better significantly reduces the risk of long-term complications. I will write about this evidence in another blog but, for now, you will have to take my word for it. As you can see above, the looping nudged the participants into this 70% mark for the duration of the study. The more interesting results were in the Time of Day analysis.

This is a study of Time in Range over the day. Comparing the Control line to the Closed Loop line we see the big difference between midnight and 9am. While there is some benefit over the rest of the day, the loop comes into its own in those early hours, presumably dealing with dawn phenomenon, although the poster did not go into details. We also see a significant narrowing of the variability during the same period as well.
Looking at the baseline measurements, at the start of the experiment compared to 16 weeks later for the control group (SAP) and the closed loop group (CLC) we see significant benefits for looping.
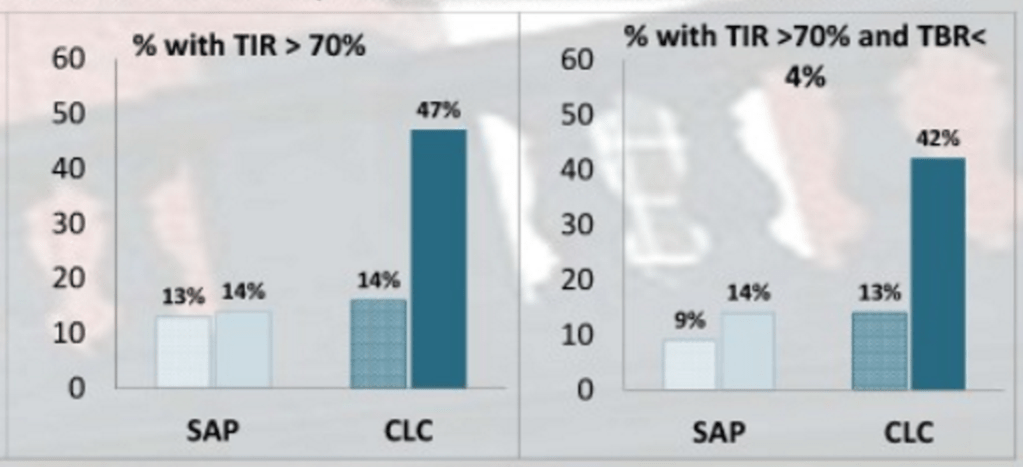
Time in Range (TIR) more than tripled and Time Below Range (TBR) also improved with a similar tripling.
Presentation 2: Nine Months Experience on Hybrid Closed Loop System in Children and Adolescents Previously Treated with Multiple Daily Injections
Presented by Goran Petrovski.
This study used the Medtronic MiniMed 670G over 9 months. The 30 participants were 7-18 years of age. There was no attrition during the study (no DKA, severe hypoglycemia, and no hospital admission) and all participants continued to use the pump (no dropouts).
As with the previous study we had a breakdown, based on the time of day.

A lot of numbers here, and I really need to write a blog on how to read scientific technobabble but, the p-values need to be less than 0.05 to make the HCL value to the left of it statistically significant. So, in other words, all the results were interesting, except for the change in weight.
Interpreting the wall of numbers, SG = Sensor Glucose Average, HbA1c is self-explanatory and TDD = Total Daily Dose (of insulin). As we can see the HbA1c dropped from 8.2 to around 6.8 and remained stable over the 9 months. From my previous analysis, we know keeping the HbA1c below 7% significantly reduces the risk of complications.
While, in the previous study, the benefits were mostly during the night, this was not the case in this study with a drop of around 50 mg/dl (2.8 mmol/L) in the sensor glucose average across the day.
The study also looked at the time in range covering the same ranges as the previous study.
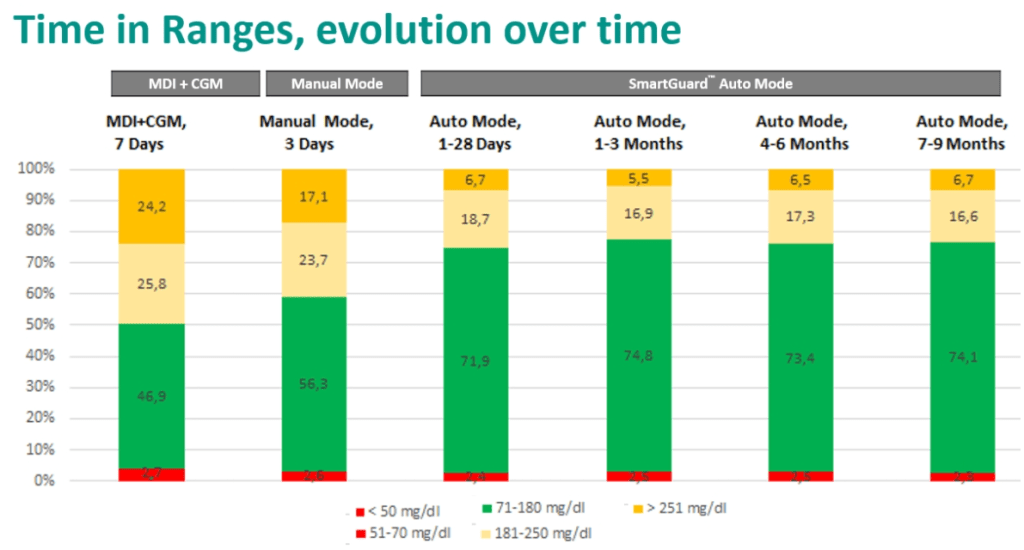
Comparing multiple daily injections (MDI) and Manual Mode i.e. no looping to the looping numbers we see a similar result to the previous study with looping nudging the participants into the all-important 70%+ zone for Time in Range. We also see no increase in Time Below Range with the ground gained coming from the high glucose levels.
Presentation 3: Glycemic Outcomes and the Importance of Active Insulin Time in the Pivotal Trial of the Minimed Advanced Hybrid Closed-Loop System
Presented by Anders Carlson.
As the title suggests, the study used the Medtronic MiniMed 780G, the model up from the 670G. Arguably the biggest difference between the two models is you can set the 780G to the more aggressive target of 5.6 mmol/L (100 mg/dL) compared to 6.7 mmol/L (120 mg/dL) for the 670G. While details of the participants were limited, there were 39 adolescents in the study which went over three months.
Again, as with the previous two studies, time of day numbers were given.

Comparing the Run-in (baseline) to the Study numbers we see that, as with the first study, there was significant improvement in the night-time numbers and a narrowing or variability, especially in the 5.6 mmol/L graph. While the first study looked at Time in Range, this one looked at the Sensor Glucose Average and while there were no ‘unicorns’, a drop of 30 mg/dL (1.7 mmol/L) is nothing to complain about.
For Time in Range, we saw similar results to the previous two studies.
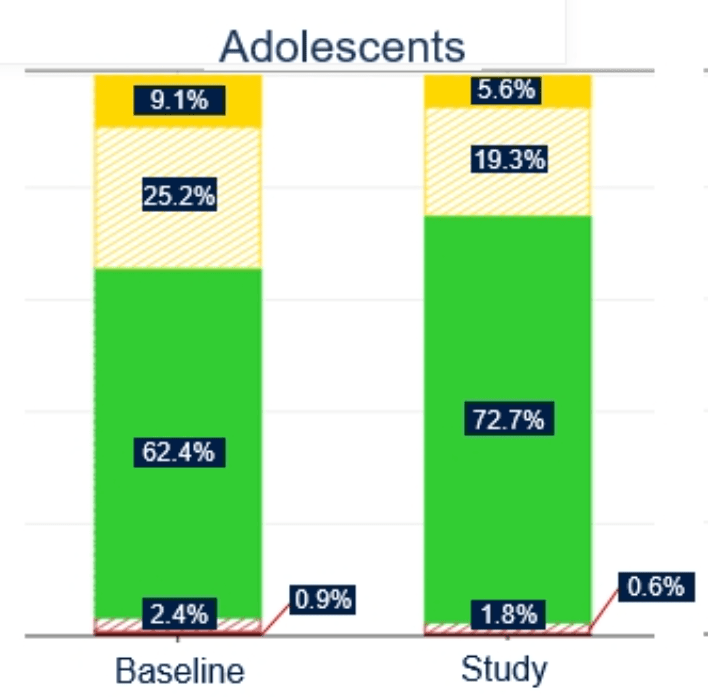
The Time in Range nudged into the 70%+ value with most of the benefit coming from the above-range time.
Presentation 4: First Home Evaluation of the Omnipod 5 Automated Insulin Delivery System, Powered by Horizon in Children with Type 1 Diabetes
Presented by Gregory Forlenza.
This case, as stated it is the Omnipod 5. The 18 children in the study were between the ages of 6 and 14 and participated over three months. There was a slight difference in this study in that different targets for the looping system were also compared.
Again, we have Time of Day numbers with, in this case, different target levels for the looping system.
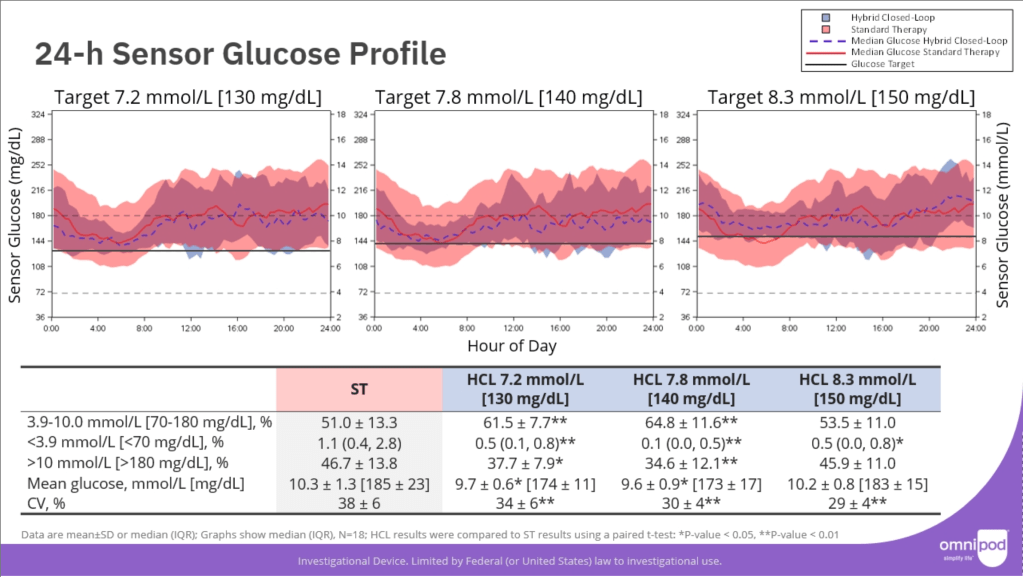
The red line is for non-looping and the blue line is looping. In this case we do not see a significant shift in the line but we do see a narrowing of the fluctuation in numbers, again, in the first third of the day supporting the notion that looping systems are good for overnight control.
For the table of numbers, anything with an asterisk is statistically significant. From this we can see that Time in Range went from 51% up to over 60% for the lower targets. This is less than the 70% seen with other systems but an improvement regardless (and the presenter was very keen to disclose that the study was done over Christmas). Time Below Range and Time Above Range were both reduced for the lower target settings.
For Time in Range,

we see that 10 out of the 18 children managed to achieve a Time in Range of greater than 70%, compared to 2 out of 18 for the non-loopers.
Also, when the more aggressive target of 6.1 mmol/L (110 mg/dL) was employed, we see the lowering of the overnight blood glucose levels we saw elsewhere and a reduction in high numbers.

tl;dr
Children can benefit greatly from looping systems compared to multiple daily injection or non-looping CGM/Pump setups. Key benefits include:
- An overall improved Time in Range (70-180 mg/dL aka 3.9-10 mmol/L) with values generally over 70% which is the critical mark to significantly reduce the risk of long term complications. The more aggressive targets (lower than 7 mmol/L aka 126 mg/dL) were the most successful at getting 70%+. Time Below Range was not always affected compared to Time Above Range which was consistently significantly reduced.
- Overnight blood glucose values were especially improved with looping both in terms of the average sensor glucose and time in range. The variability of the numbers was also improved with looping.
- The results were largely independent of the looping system employed; the benefits are down to the overall technology, not any one company’s version of it.
