I posted this Tweet based on one of the presentations at EASD 2020.
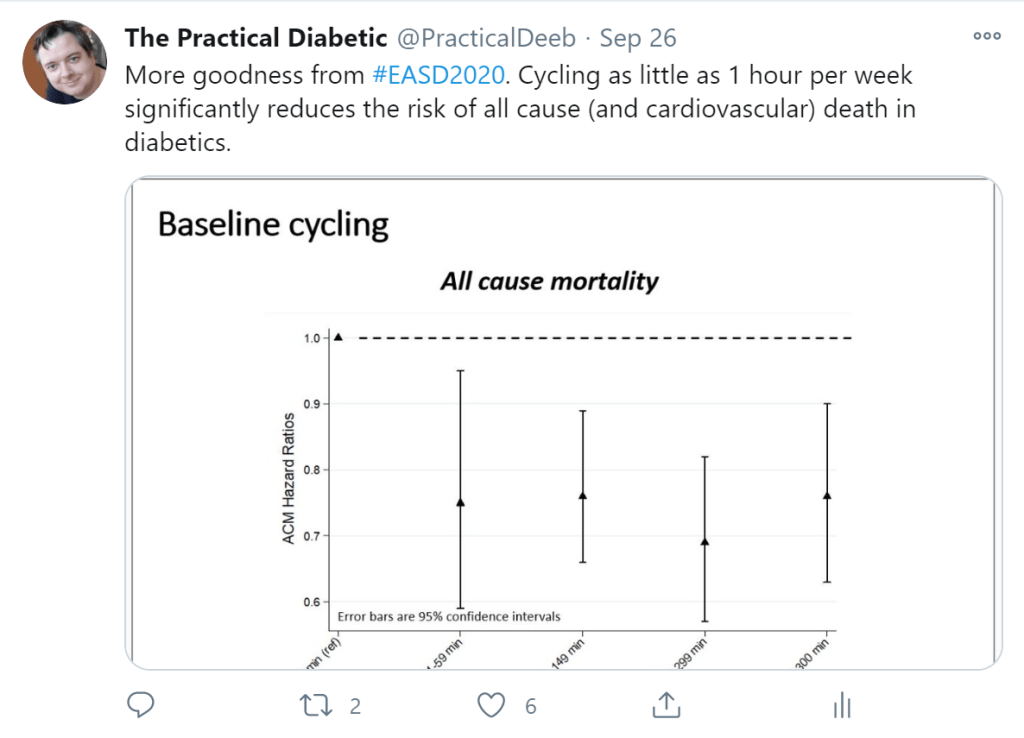
It is worth going through some of the details because it seems incredible that as little as one hour a week of cycling really reduces all-cause mortality by more than 20% in diabetics. It is also a great study to see the limitations of research and statistics. As usual, if you want to cut to the chase, head on over to the tl;dr section.
Details of the Study
Presented by Mathias Ried-Larsen, data was taken from the “European Prospective Investigation into Cancer and Nutrition” (EPIC). This is a massive study across 10 European countries with over half a million participants looking at factors such as diet, environment, lifestyle, and chronic disease.
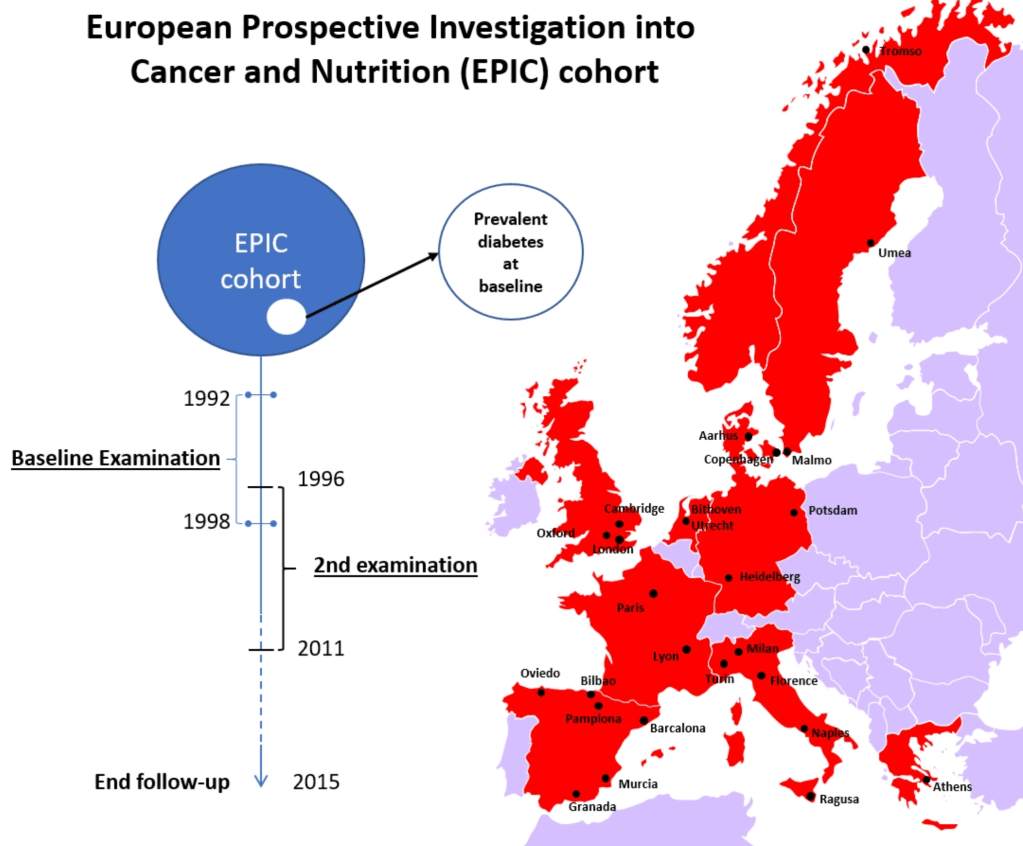
They took the data and filtered it to people with diabetes at the start of the EPIC study and for which relevant data had been recorded. This brought the number of participants down to 7,513 of which 63% were confirmed to have diabetes with the others being self-reported. A second cohort was considered at the second examination point to see how a change in cycling habits changed mortality rates. This second group comprised of 5,506 people.
The forms of mortality looked at were all-cause mortality (dying for any reason) and cardiovascular mortality (presumably because it is a common killer and one which is a higher risk in diabetics).
Looking at other factors of the diabetes group, it was seen that the participants were mostly middle-aged and overweight, and most did no cycling at all.

Despite the shrinking cohort numbers, they still obtained the graph I tweeted.

The bars on the four points can be thought of as the error in the value (with this level of error we are 95% confident the value is correct, equivalent to a p-value of 0.05 and is considered statistically significant). So, for example, if I do between 1 and 59 minutes of cycling in a week, my risk of all-cause mortality (ACM) drops to somewhere between 60% and 95% of the baseline risk.
The presenter claimed the covariates (other factors we know about the people) were statistically removed from affecting the numbers attributed to the cycling. So, for example, given women generally live longer than men, this could have an effect on the results so this was accounted for when looking at the results.
The presenter further claimed that there was a j-curve relationship with the data i.e. the benefits are reduced at the 300+ minute mark. To explore this, rather than bucket the cycling times into four groups, they looked at the cycling times as they were i.e. a continuous spread of values between zero and nine hours of cycling per week.

While there is a curve with a maximum benefit around 4-5 hours, there is a fairly wide error margin (UCL = Upper confidence level, LCL = Lower confidence level i.e. the upper and lower values with a 95% confidence of being right). In other words, while the curve seems to head up after five hours, the error means it could just as easily be heading down to between 0.6 to 0.7. Similar results were obtained when cardiovascular mortality was specifically examined.
Next was the review of the effect of changing cycling habits.
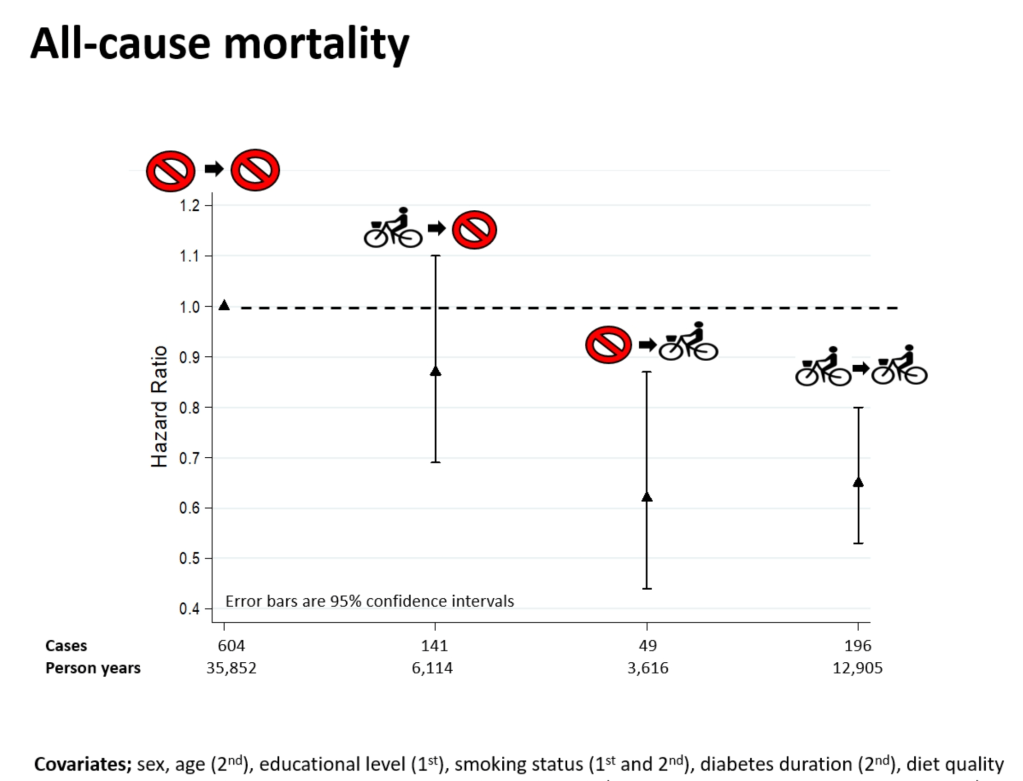
The takeaway here is starting to cycle yields at least a 10% reduction in all-cause mortality while maintaining a cycling habit reduces risk by between 20% and close to 50%. For cardiovascular risk, maintaining a cycling habit had slightly better results with the risk reducing by 30-60%.
Recognised Limitations
The presentation did talk at some of the limitations:
- Confounding factors: As mentioned they looked at the influence other factors, such as age and smoking had but claim their results still stand
- Medication: There was no information on the medications being used by the diabetics and the effect they would have on mortality
- Underlying disease leading to less exercise and more mortality (reverse causation): As with the confounding factors, they looked at the potential influence and ruled it out as affecting the results
- There was no distinction in EPIC between Type 1 and Type 2 diabetes so no conclusions between the Types could be made but it is assumed the distribution in the study is close to the general population and, therefore 80-90% of the cohort was Type 2
tl;dr
For middle-aged Western European diabetics, the study showed:
- Cycling reduces all-cause mortality and cardiovascular mortality
- The level of benefit is harder to quantify but, the best benefit was shown to be at around 4-5 hours per week of cycling where the reduction in risk was roughly between 20-40%. Additional cycling may be of benefit but the error margins were too high to confirm this one way or the other
- Starting a cycling habit or maintaining one shows benefit with the most benefit being for someone who maintain a cycling habit with the reduction in risk being between 20-50% for all-cause mortality and 30-60% for cardiovascular mortality
- There was no distinction of Type so it is best to assume these results apply most strongly to Type 2 but I can see no reason why it would be different to Type 1s except for the additional risk of hypo if insulin dependent

One thought on “EASD 2020: Is Cycling Good For Diabetics?”