I have just returned from ATTD 2024 in Florence, Italy thanks to dedoc. ATTD (Advanced Technologies and Treatments for Diabetes) is one of the largest diabetes conferences in Europe. While the formal focus is on technology and new medications, the research coverage was quite broad. for example, I had a poster at the conference talking about motivation theory and its application in the doctor’s office.

I also presented on the petition to guarantee the humanitarian supply of medication, including insulin, to civilians in war-affected areas, in line with documents such as the Geneva Conventions. If you are interested in signing the petition, please go to https://www.change.org/insulinconsensus

Image care of https://twitter.com/1derfultype
So What Did I Learn?
In the spirit of Michelle Law’s Top Ten Takeaways and dedoc’s #PayItForward, I thought I would list the topics presented which piqued my interest.
Non-Invasive Glucose Measurement
In the expo area of the conference were a lot of companies looking to measure glucose in non-invasive ways, such as through saliva or with various electromagnetic waves scanning the skin. The measure of choice for determining accuracy for these systems is MARD (Mean Absolute Relative Difference). Generally speaking, a MARD less than 10% is considered accurate enough to inform insulin delivery i.e. be included in a bolus/looping system.
To understand how MARD can be manipulated look no further than Tim Street‘s excellent reviews of CGMs and how their accuracy is assessed, such as this one. However, even with the ability to artificially lower the numbers, the lowest MARDs being reported were in the low teens so, at least for now, finger-pricking and CGM insertion will need to continue.
TITR Gets More Coverage
At last year’s ATTD blog article, I mentioned Professor Thomas Danne pushing for Time in Tight Range (TITR, 3.9-7.8 mmol/L = 70-140mg/dL) rather than the usual Time in Range (TIR, 3.9-10 mmol/L = 70-180mg/dL) because it is a better predictor of the onset of Stage 3 diabetes and a better target for minimising the risk of long-term complications. In short, he suggested the evidence-based 50% TITR was a better goal than the consensus-based 70% TIR.
At this year’s ATTD, there was more talk of TITR and it is clear it is becoming an accepted standard in academic research. Some of the other dedoc voices expressed concern that a stricter range could lead to more pressure on people with diabetes (PWD) to ‘succeed’. While I am sympathetic to this concern, I would prefer my targets to be evidence-based but, to make sure people do not over-obsess on the numbers, perhaps a multi-target strategy should be considered with both quantitative and qualitative measures, aligned to the PWD’s goals.

Image care of https://twitter.com/Drhkakturk
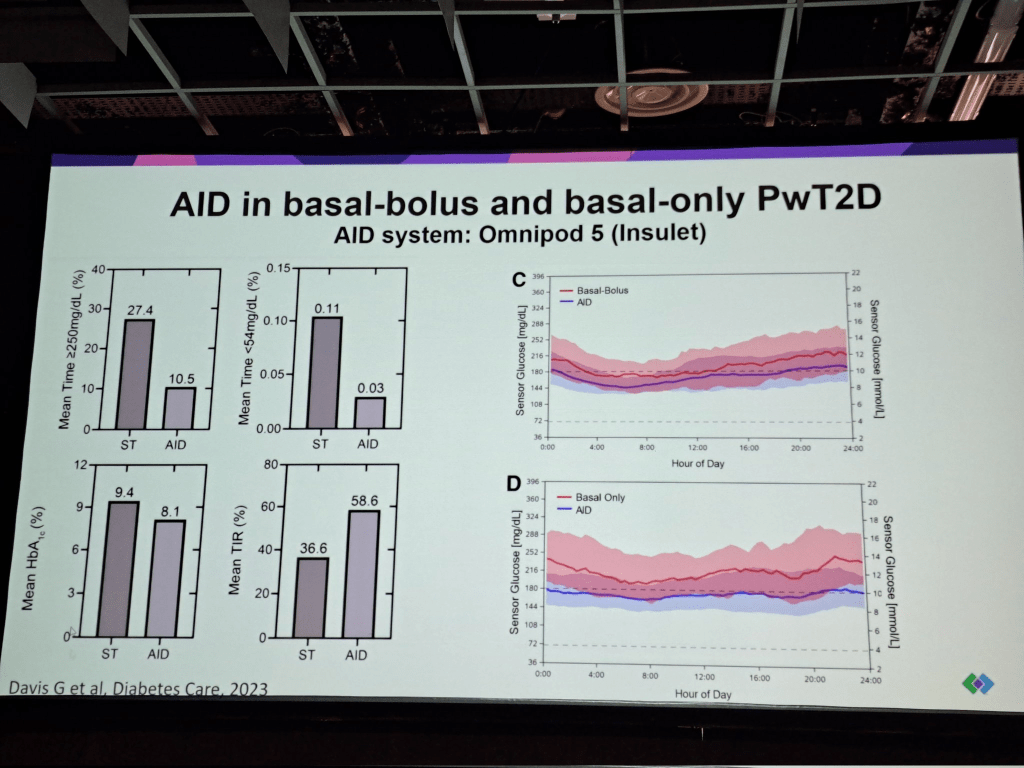
Continuous Glucose Monitors (CGMs) and Looping for Type 2 Diabetes
Historically, CGMs and Looping technology has been considered a type 1 tool. However, there are people with type 2 diabetes who require insulin and, from a common-sense perspective, based on the type 1 evidence, it makes sense they would also benefit from the technology. ATTD 2024 presented a variety of studies which confirmed this. Given the type 2 diabetes market is literally ten times the size of the type 1 diabetes market, it makes sense that diabetes tech. companies would pursue it.

Continuous Ketone Monitoring
The idea of monitoring ketones continuously, as well as blood sugar was also presented. It was shown that rising ketones can be used to predict hyperglycemia spikes and potentially predict DKA before it becomes dangerous. Abbott even went as far as to talk about a future all-in-one sensor which would track both in the one unit. Where I see this being useful is providing additional information for looping systems, to predict exercise, better handle ketogenic diets and SLGT2i medications.



GLP1s for Obesity Management
Drugs like semaglutide (Ozempic/Wegovy) are “single agonist GLP1s”: they bind to cells and trigger the same response as GLP1s in the body. The next generation of these drugs are in trials, referred to as double or triple agonists i.e. they activate more receptor sites. The upshot is they are more effective than their single agonist predecessors. How effective? Trials are reporting people losing 20-30% of their weight on the drugs which is incredibly powerful.

LADA Confirmed as a Distinct Phenotype and “Curable”
Perhaps because ATTD was in Italy, the home of Professor Raffaella Buzzetti, one of the leading authorities on LADA, there was substantially more coverage of LADA than I had seen in previous conferences. Professor Buzzetti presented evidence showing LADA is a distinct phenotype of type 1 diabetes (a distinct disease that presented differently) and confirmed that, with immune intervention drugs such as Teplizumab, it may be possible to indefinitely hold off LADA from becoming insulin dependent i.e. a cure.

#LanguageMatters Becomes #DeliveryMatters
One presentation talked at, not so much the words we use in speaking with people with diabetes but, how we talk to them i.e. with empathy and respect. This is a shift in the #LanguageMatters movement but a welcome one.

Patient Reported Outcomes (PROs) and Measures (PROMs)
This had been touched upon in previous conferences but, again, seemed to have more prominence at ATTD 2024. In short, PROs are outcomes which are important to the person with diabetes, more than the clinician.

PROMs are the measures to assess them. At this stage, while there are PROM questionnaires being used in research, their efficacy is not strongly validated, and there is concern they are being used without a purpose in mind.
“Artificial Intelligence is not Ready for Primetime”
The use of artificial intelligence (AI) systems to provide guidance to people with diabetes in their daily management and in providing general advice on diabetes was discussed and considered not ready for general use because of ‘hallucinations’ (false facts incorrectly inferred by the AI engine which need to be verified by the user). Examples cited included mixing up mmol/L with mg/dL which could be disastrous in the context of giving insulin administration advice.
This being said, the potential was recognised once obstacles were addressed.


Tips and Tricks for People with Type 2 Diabetes
One study was presented which showed, even if the types of food a person with type 2 diabetes is eating does not change, intermittent fasting will still reduce their HbA1c. This is intuitively obvious, but it is good to have the evidence to back it up.

Another study showed 2.5-6.5 hours of exercise per week helps people with early stages of type 2 diabetes inproves beta cell function.

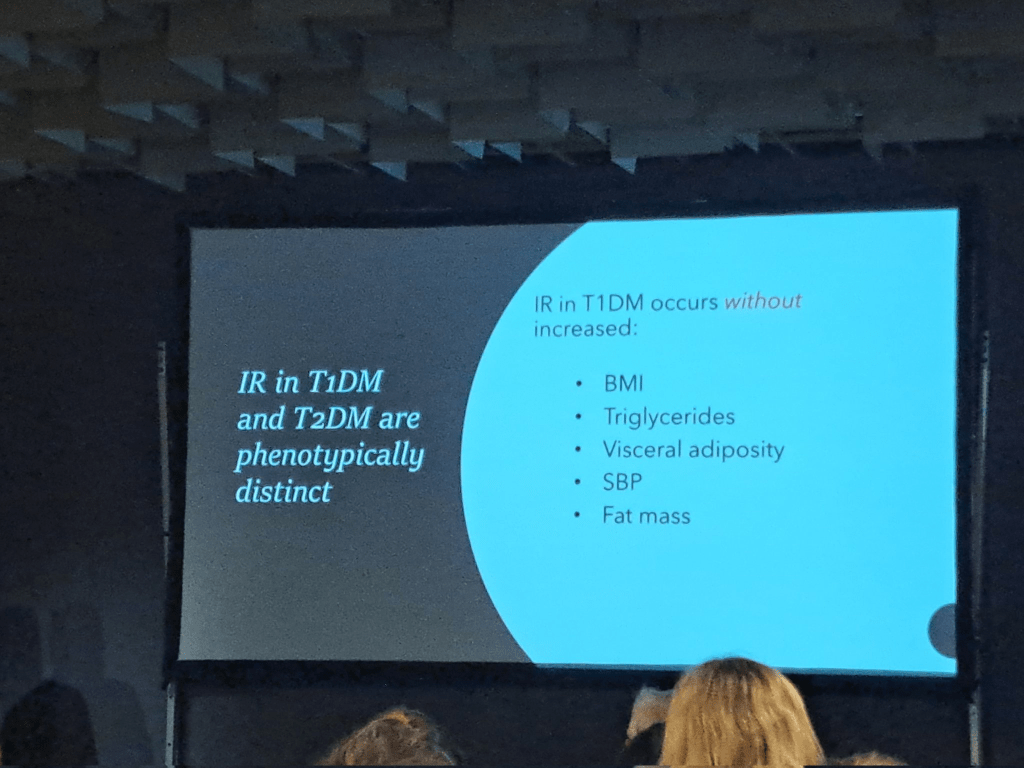
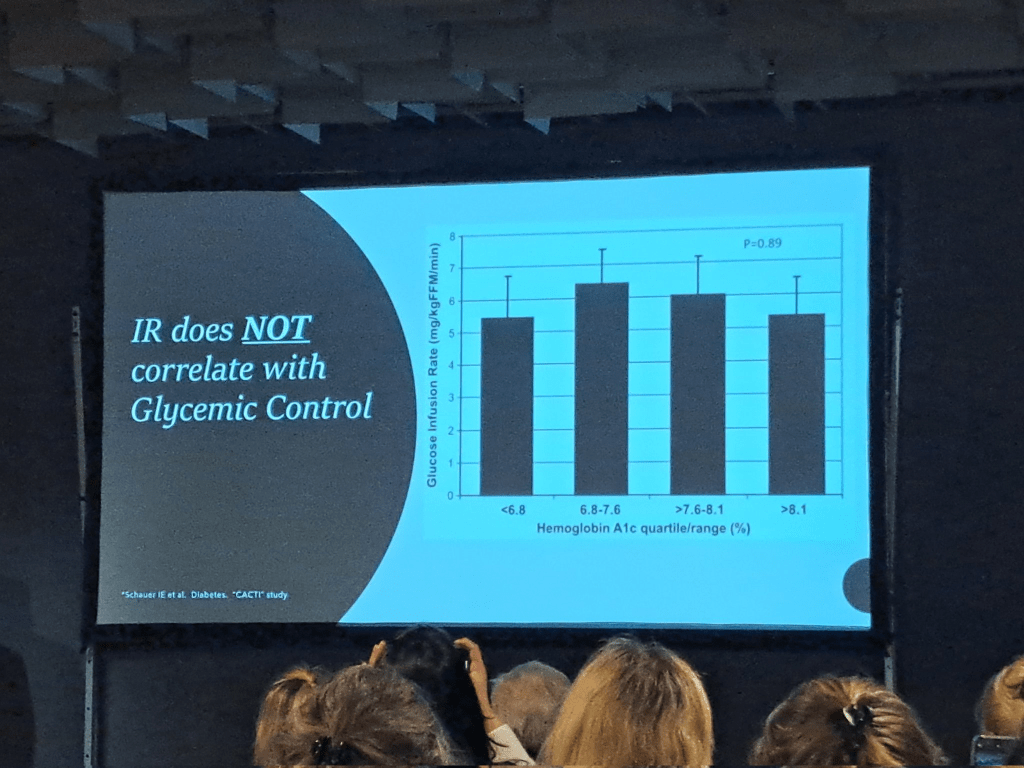
Type 1s have Insulin Resistance Too!
Rendering the term “double diabetes” somewhat redundant, it was shown that people with type 1 diabetes also have insulin resistance which, in their case, is driven by the insulin they inject and is independent of factors such as weight or glycemic control. Low carb was mentioned as one lever to pull in managing it.



Thank You dedoc!!
If you are interested in also attending these kinds of conferences, I highly recommend going to the dedoc web site and applying for one of their scholarships. They cover flights, accommodation, and conference registration. Am I one of these infamous “paid diabetes advocates” we hear so much about on social media? I do not think so. I still had to take leave from work and cover other expenses out of my own pocket. My bank account is no richer for the experience but my knowledge of where the research is heading certainly is and the friendships made with other diabetes advocates around the world are priceless. This is why I continue to apply for the scholarships for myself and for the communities I serve.

